
The Complete Guide to Healing From Sexual Trauma.trauma-informed Sex therapy in scottsdale, az
Understanding the Lasting Impact of Sexual Trauma on Your Mind, Body, Relationships, and Sexuality
By Holly Nelson, LPC | EMDR Certified Therapist | AASECT Certified Sex Therapist (In Progress)
Introduction
Sexual trauma can affect every part of a person's life. It can change the way you think, feel, relate to others, experience your body, and connect with intimacy. Whether the trauma happened recently or many years ago, its effects can continue long after the event itself has ended.
If you're reading this guide, you may be searching for answers to questions like:
Why do I still think about what happened?
Why do I freeze during intimacy?
Why has my sex drive changed?
Why do I panic when my partner touches me?
Why do I feel disconnected from my body?
Will I ever enjoy sex again?
Can sex therapy really help me heal?
If you've asked yourself any of these questions, you are not alone.
Sexual trauma affects millions of people each year, and there is no "right" or "wrong" way to respond to it. Some survivors develop symptoms of post-traumatic stress disorder (PTSD), while others experience anxiety, depression, panic attacks, chronic pain, difficulty trusting others, or changes in their sexual desire and functioning. Many survivors also experience trauma responses they don't immediately recognize, such as dissociation, emotional numbness, hypervigilance, shame, guilt, or feeling disconnected from their bodies.
The good news is that healing is possible.
Over the past several decades, researchers have learned that trauma changes the brain and nervous system—but they have also discovered something equally important: the brain has the ability to heal. Through neuroplasticity, the brain can form new pathways that support recovery, safety, connection, and resilience. Evidence-based treatments such as Eye Movement Desensitization and Reprocessing (EMDR), trauma-focused therapy, sex therapy, Cognitive Processing Therapy (CPT), Trauma-Focused Cognitive Behavioral Therapy (TF-CBT), somatic therapies, and other trauma-informed approaches have helped countless survivors reduce symptoms and reclaim their lives.
This guide was created to be a comprehensive, evidence-based resource for anyone wanting to better understand sexual trauma and the healing process. Whether you are a survivor, the partner of a survivor, a family member, or simply looking to learn more, you'll find practical information supported by current psychological research and trauma-informed clinical practice.
Throughout this guide, you'll learn:
What sexual trauma is and the many forms it can take.
How trauma affects the brain, nervous system, and body.
Why trauma can impact relationships, intimacy, and sexual functioning.
Common trauma responses such as fight, flight, freeze, fawn, and dissociation.
Why survivors often experience low libido, painful sex, erectile dysfunction, difficulty reaching orgasm, or fear of intimacy.
Evidence-based treatments for sexual trauma, including EMDR therapy, trauma therapy, pelvic floor physical therapy, sex therapy, and other proven approaches.
Practical strategies for rebuilding safety, trust, connection, intimacy, and pleasure.
Answers to the most common questions people ask about healing from sexual trauma.
One of the most important things to know is this: your reactions make sense.
Many survivors blame themselves for how they responded during or after the trauma. You may wonder why you froze, why you didn't fight back, why you stayed in the relationship, or why your body reacted in ways you didn't expect. These questions are incredibly common, and the answers lie in how the brain and nervous system are designed to protect us during overwhelming experiences.
Healing does not mean forgetting what happened. It does not mean pretending the trauma never existed. Healing means understanding what happened to your mind and body, learning new ways to feel safe, reconnecting with yourself, and discovering that your past does not have to define your future.
Recovery is rarely a straight line. There will likely be moments of growth, setbacks, victories, and challenges along the way. But with the right support, healing is absolutely possible. Many survivors go on to build healthy relationships, experience fulfilling intimacy, reconnect with pleasure, and create lives that are no longer controlled by trauma.
Whether the trauma happened weeks ago or decades ago, whether you've never told anyone or you've been in therapy for years, this guide is for you. My hope is that by the time you finish reading, you'll have a better understanding of what sexual trauma is, why your mind and body respond the way they do, and the many evidence-based tools available to support your healing.
You deserve safety. You deserve healing. And you deserve relationships and intimacy that are built on trust, respect, and choice.
Welcome. I'm honored you're here.
Table of Contents
Part 1: Understanding Sexual Trauma
What Is Sexual Trauma?
Types of Sexual Trauma
Childhood Sexual Abuse
Adult Sexual Assault
Marital or Intimate Partner Rape
Sexual Coercion or Pressure
Stealthing (Non-Consensual Condom Removal)
Drug- or Alcohol-Facilitated Sexual Assault
Sexual Harassment
Medical or Gynecological Trauma
Religious or Purity Culture Trauma
Military Sexual Trauma
Human Trafficking and Sexual Exploitation
Birth Trauma
Image-Based Sexual Abuse
Online Sexual Abuse and Grooming
Reproductive Coercion
Does My Experience "Count" as Trauma?
Common Myths About Sexual Trauma
Part 2: How Trauma Changes the Brain and Body
The Survival Response
Fight
Flight
Freeze
Fawn
Collapse
The Brain on Trauma
The Window of Tolerance
The Nervous System and Trauma
Why Trauma Responses Are Not a Choice
Populations with Special Considerations
LGBTQIA+
Male Survivors
Sex Workers
Survivors with Disabilities
Part 3: How Sexual Trauma Can Affect Your Life
Emotional Effects
Physical Effects
Relationship Effects
Sexual Effects
Mental Health After Trauma
Part 4: Why Sex Can Feel Different After Trauma
Changes in Sexual Desire
Pain During Sex
Difficulty Becoming Aroused
Difficulty Reaching Orgasm
Erectile Dysfunction After Trauma
Dissociation During Sex
Feeling Numb or Disconnected
Hypersexuality as a Trauma Response
Feeling Guilty for Enjoying Sex Again
Part 5: Understanding Triggers
What Is a Trigger?
Common Sexual Trauma Triggers
Trigger vs. Actual Danger
Managing Triggers
Part 6: Dissociation
What Is Dissociation?
Why Dissociation Happens
Signs of Dissociation
Grounding Techniques
Reconnecting With Your Body
Part 7: Healing Is Possible
What Recovery Really Looks Like
Neuroplasticity and Healing
Building Safety Again
What Progress Can Look Like
Part 8: Evidence-Based Treatments for Sexual Trauma
EMDR Therapy
Somatic Therapy
Cognitive Processing Therapy (CPT)
Trauma-Focused Cognitive Behavioral Therapy (TF-CBT)
Prolonged Exposure Therapy
Internal Family Systems (IFS)
Sex Therapy
Pelvic Floor Physical Therapy
Medication
Part 9: Rebuilding Intimacy
Reconnecting With Yourself
Taking Sex Off the Table
Sensate Focus
Expanding Intimacy Beyond Penetration
Communicating Boundaries
Rebuilding Trust
Returning to Sexual Activity
Part 10: What Partners Should Know
How Trauma Affects Relationships
Supporting a Survivor
Helpful Things to Say
Things to Avoid
Navigating Consent Together
Patience During Healing
Part 11: Healing Your Relationship With Your Body
Body Image After Trauma
Body Neutrality and Self-Compassion
Mindfulness and Movement
Reconnecting With Pleasure
Reclaiming Your Body
Part 12: Frequently Asked Questions
Can sexual trauma cause low libido?
Can sexual trauma cause painful sex?
Can sexual trauma cause erectile dysfunction?
Can sexual trauma cause vaginismus?
Can sexual trauma cause difficulty orgasming?
Why do I dissociate during sex?
Why do I freeze during sexual assault?
Can EMDR help sexual trauma?
How long does healing take?
Can I ever enjoy sex again?
Is it normal to avoid sex after assault?
Can men experience sexual trauma?
Why do I blame myself?
Why can't I remember everything?
Is hypersexuality a trauma response?
Does everyone develop PTSD after sexual trauma?
Can therapy still help years later?
Part 13: Key Takeaways
What to Remember About Healing From Sexual Trauma
Part 14: Next Steps If You're Ready for Help
When to Seek Professional Support
Finding a Trauma-Informed Therapist
Finding an EMDR Therapist
Finding a Sex Therapist
What to Expect During Your First Session
About the Author
References
Part 1: Understanding Sexual Trauma
What Is Sexual Trauma?
Sexual trauma is any unwanted, non-consensual, or coercive sexual experience that overwhelms a person's ability to cope and leaves lasting emotional, psychological, physical, or relational effects. While many people think sexual trauma only refers to rape or sexual assault, it can result from a wide range of experiences that violate a person's sense of safety, autonomy, or bodily boundaries.
Sexual trauma is not defined solely by what happened—it is also shaped by how the experience affected you. Two people may experience similar events but have very different responses. One person may recover relatively quickly, while another may experience lasting symptoms that affect their daily life, relationships, and sexual well-being. Neither response is "right" or "wrong." Trauma is highly individual.
At its core, sexual trauma occurs when a sexual experience is experienced as frightening, overwhelming, coercive, or violating. This can happen because consent was never given, consent could not legally or ethically be given, consent was withdrawn but not respected, or someone felt pressured, manipulated, threatened, or unable to say no.
Sexual trauma can happen to anyone, regardless of age, gender, sexual orientation, race, culture, religion, or relationship status. It affects children, adolescents, and adults. It happens in dating relationships, marriages, families, schools, workplaces, religious communities, military settings, healthcare environments, and among strangers. Most importantly, sexual trauma is never the survivor's fault.
Sexual trauma can have both immediate and long-term effects. Some people experience symptoms right away, while others may not notice the impact until months or even years later. Common effects include anxiety, depression, post-traumatic stress disorder (PTSD), nightmares, panic attacks, shame, guilt, difficulty trusting others, emotional numbness, hypervigilance, dissociation, chronic pain, and changes in sexual desire or functioning. Survivors may also experience painful sex, vaginismus, erectile dysfunction, difficulty reaching orgasm, avoidance of intimacy, or fear of physical touch.
One of the most important things to understand is that trauma is not a sign of weakness. Your brain and nervous system are designed to protect you during overwhelming experiences. Many of the symptoms survivors experience—including freezing during an assault, feeling emotionally numb afterward, or becoming easily startled—are normal survival responses to abnormal circumstances.
Although sexual trauma can have profound effects, it does not have to define the rest of your life. Decades of research show that the brain and nervous system can heal. Evidence-based treatments such as Eye Movement Desensitization and Reprocessing (EMDR), trauma-focused psychotherapy, sex therapy, Cognitive Processing Therapy (CPT), and other trauma-informed approaches have helped countless survivors reduce symptoms, rebuild trust, reconnect with their bodies, and experience healthy intimacy again.
Understanding what sexual trauma is—and recognizing that your reactions make sense—is often the first step toward healing.

Types of sexual trauma:
Childhood Sexual Abuse
Childhood sexual abuse (CSA) is any sexual activity involving a child that they cannot understand, consent to, or legally agree to. Because children are still developing emotionally, cognitively, and physically, they are unable to give informed consent to sexual acts with an adult or an older person in a position of power. Childhood sexual abuse is a violation of a child's safety, trust, and bodily autonomy.
Childhood sexual abuse can involve physical contact, such as touching or penetration, but it does not have to. It may also include exposing a child to sexual acts, showing them pornography, encouraging them to participate in sexual conversations or behaviors, taking or sharing sexual images of a child, online sexual exploitation, or grooming. Abuse can occur once or repeatedly and may involve manipulation, threats, secrecy, gifts, or emotional coercion rather than physical force.
One of the most difficult realities about childhood sexual abuse is that the person responsible is often someone the child knows and trusts. This may include a family member, caregiver, family friend, coach, teacher, religious leader, neighbor, or another trusted adult. Because of this, many survivors experience confusion, guilt, loyalty conflicts, or fear about telling someone what happened.
Many survivors do not disclose childhood sexual abuse until adulthood. Some never tell anyone. Others may not fully recognize that what happened was abuse until years later. This is especially common when grooming, manipulation, or emotional dependence were involved. Delayed disclosure does not make someone's experience any less real or valid.
The effects of childhood sexual abuse can continue into adulthood in many different ways. Some survivors experience anxiety, depression, post-traumatic stress disorder (PTSD), shame, low self-esteem, difficulty trusting others, or challenges with emotional regulation. Others may experience difficulties in romantic relationships, fear of intimacy, chronic pain, dissociation, or changes in sexual functioning such as low libido, painful sex, erectile dysfunction, difficulty reaching orgasm, or avoiding sexual intimacy altogether. Some survivors may become hypersexual, while others lose interest in sex completely. Every survivor's response is unique.
It is also important to understand that many of these responses are survival adaptations. Children often cope in the only ways available to them. They may freeze, comply, dissociate, minimize what happened, or blame themselves in order to survive overwhelming experiences. These responses are not signs of weakness—they are signs of a nervous system doing its best to protect a child in an unsafe situation.
Although childhood sexual abuse can have lifelong effects, healing is possible. Research consistently shows that trauma-informed therapy can help survivors process traumatic memories, reduce symptoms, rebuild a sense of safety, and develop healthier relationships with themselves and others. Evidence-based treatments such as Eye Movement Desensitization and Reprocessing (EMDR), Cognitive Processing Therapy (CPT), Trauma-Focused Cognitive Behavioral Therapy (TF-CBT), somatic therapies, and sex therapy have helped many survivors move toward recovery.
Healing does not erase the past, but it can reduce the power the past has over your present. With support, many survivors go on to experience healthy relationships, fulfilling intimacy, greater self-compassion, and a renewed sense of control over their lives.
Adult Sexual Assault
Adult sexual assault is any sexual act or sexual contact that occurs without a person's freely given, informed, and voluntary consent. It can happen to people of any gender, sexual orientation, race, culture, or relationship status. Sexual assault may be committed by a stranger, but it is far more common for the perpetrator to be someone the survivor knows, such as a dating partner, spouse, friend, coworker, acquaintance, family member, or someone in a position of trust or authority.
Many people picture sexual assault as a violent attack by a stranger. While those assaults do occur, they represent only a portion of sexual assaults. In reality, sexual assault often happens in familiar settings and may involve manipulation, coercion, intimidation, threats, alcohol or drugs, or taking advantage of someone who is asleep, unconscious, or otherwise unable to consent.
The defining feature of sexual assault is not the amount of physical force used—it's the absence of consent.
Survivors often blame themselves because they didn't fight back, scream, or physically resist. However, trauma research has shown that many people automatically enter survival responses such as freezing, complying, dissociating, or becoming unable to speak when faced with overwhelming danger. These responses are controlled by the nervous system and are not conscious choices.
What's the Difference Between Sexual Assault and Rape?
The terms sexual assault and rape are often used interchangeably, but they are not always defined the same way.
Sexual assault is a broad term that refers to many forms of unwanted sexual contact or sexual activity without consent. Depending on the laws where someone lives, sexual assault may include:
Unwanted sexual touching
Forced kissing
Groping
Attempted rape
Rape
Being forced to perform sexual acts
Sexual acts committed against someone who is asleep, unconscious, intoxicated, or otherwise unable to consent
Some forms of reproductive coercion or sexual violence
Rapegenerally refers to a form of sexual assault involving non-consensual penetration. The exact legal definition varies by country and state, but it commonly includes vaginal, anal, or oral penetration without consent.
In other words:
All rape is sexual assault, but not all sexual assault is rape.
Because legal definitions differ across jurisdictions, this guide uses the broader term sexual assault when discussing trauma and recovery. Regardless of the legal terminology, any sexual experience that occurred without your freely given consent can have a significant emotional and psychological impact.
Consent Matters
Consent is more than simply the absence of "no."
Consent is:
Freely given
Informed
Specific to the activity
Ongoing throughout the encounter
Able to be withdrawn at any time
Someone cannot legally or ethically consent if they are:
Asleep
Unconscious
Extremely intoxicated or incapacitated
Threatened or physically forced
Manipulated through fear or coercion
Afraid of the consequences of saying no
Consent to one sexual activity does not automatically mean consent to another. Likewise, consenting in the past does not mean someone consents in the future.
Being married, dating, or in a long-term relationship does not eliminate the need for consent.
Common Reactions After Sexual Assault
Every survivor responds differently. Some people experience overwhelming distress immediately after the assault, while others feel numb or believe they are "fine" until symptoms appear weeks, months, or even years later.
Common reactions include:
Shock or disbelief
Fear or anxiety
Shame or embarrassment
Guilt or self-blame
Anger
Emotional numbness
Hypervigilance
Panic attacks
Nightmares
Difficulty sleeping
Depression
Difficulty trusting others
Avoidance of reminders of the assault
Dissociation
Changes in sexual desire or functioning
Many survivors also experience changes in intimacy. They may avoid sexual contact, experience pain during sex, have difficulty becoming aroused or reaching orgasm, develop erectile dysfunction, or feel emotionally disconnected during intimacy. Others may experience an increase in sexual behavior as a way of coping or attempting to regain a sense of control. There is no single "correct" trauma response.
Common Myths About Sexual Assault
Unfortunately, many harmful myths continue to discourage survivors from seeking support.
Myth: "If I didn't fight back, it wasn't really assault."
Fact: Freezing is one of the most common survival responses during trauma. Many survivors are physically unable to move or speak because their nervous system automatically shifts into survival mode.
Myth: "It only counts if a stranger attacked me."
Fact: Most survivors know the person who assaulted them. Sexual assault frequently occurs within dating relationships, marriages, friendships, workplaces, schools, and families.
Myth: "I was drinking, so it was my fault."
Fact: Choosing to drink alcohol is never the same as consenting to sexual activity. Responsibility always belongs to the person who chose to violate someone else's boundaries.
Myth: "My body responded, so I must have wanted it."
Fact: The body can respond automatically to sexual stimulation, even during assault. Physical arousal is a biological reflex—not evidence of consent, enjoyment, or desire.
Myth: "It happened years ago. I should be over it."
Fact: Trauma has no expiration date. Many survivors seek help years or even decades later, especially when symptoms begin affecting relationships, intimacy, or daily life.
Marital or Intimate Partner Rape
Marital or intimate partner rape is any form of non-consensual sexual activity that occurs within a marriage, dating relationship, or other intimate partnership. Although many people assume that marriage or a committed relationship automatically implies ongoing consent to sex, this is not true. Every person has the right to choose if, when, and how they engage in sexual activity, regardless of their relationship status.
Consent must be freely given every time. Being married, living together, dating, or having had consensual sex in the past does not mean someone has permanent consent to future sexual activity. A person can say "no," change their mind, withdraw consent at any point, or choose not to engage in sexual activity for any reason.
Marital rape has historically been misunderstood and minimized. In many countries, including parts of the United States, marital rape was not legally recognized until relatively recently. Harmful beliefs such as "spouses can't rape each other" or "it's your duty to have sex with your partner" have contributed to survivors feeling confused, ashamed, or unsure whether what happened to them was abuse.
Today, marital and intimate partner rape are recognized as forms of sexual violence.
What Can Marital or Intimate Partner Rape Look Like?
Many survivors do not immediately recognize what they experienced because it often looks different from the stereotypes portrayed in movies or the media. It may involve physical force, but it can also involve coercion, intimidation, manipulation, or exploiting a partner's vulnerability.
Examples may include:
Forcing a partner to have sex after they have said "no."
Continuing sexual activity after consent has been withdrawn.
Using threats, intimidation, or fear to obtain sex.
Pressuring a partner until they "give in."
Having sex with a partner who is asleep, unconscious, heavily intoxicated, or otherwise unable to consent.
Physically restraining a partner during sexual activity.
Ignoring a partner's pain or distress during sex.
Forcing specific sexual acts that the partner has refused.
Using financial control, immigration status, children, or emotional manipulation to pressure a partner into sexual activity.
In abusive relationships, sexual violence often occurs alongside emotional abuse, verbal abuse, financial abuse, coercive control, or physical violence. These patterns can make it even more difficult for survivors to recognize the abuse or leave the relationship safely.
Sexual Coercion vs. Consent
Not every unwanted sexual experience involves physical force.
Some survivors experience sexual coercion, which occurs when someone feels pressured, manipulated, guilted, threatened, or emotionally worn down into sexual activity they do not freely want. Examples include statements such as:
"If you loved me, you would."
"You never want to have sex with me."
"I'm your spouse—you owe me."
"I'll leave you if you don't."
"I'll find someone else."
Repeated pressure can make someone feel that saying "yes" is easier or safer than continuing to refuse.
Healthy consent is enthusiastic, freely given, and made without fear of punishment, rejection, manipulation, or retaliation.
Why Survivors Often Stay
One of the most common questions survivors ask themselves is, "Why didn't I leave?"
The answer is often far more complex than people realize.
Survivors may stay because they:
Love their partner.
Hope things will improve.
Fear retaliation or increased violence.
Have children together.
Depend on their partner financially.
Fear losing housing or stability.
Feel ashamed or embarrassed.
Have been isolated from friends and family.
Have been told repeatedly that the abuse is their fault.
Worry no one will believe them.
Trauma bonding, fear, manipulation, and coercive control can make leaving extremely difficult. Staying in an abusive relationship is not a sign of weakness. It often reflects the complex realities survivors face when trying to protect themselves and those they love.
The Effects of Marital or Intimate Partner Rape
The emotional impact of sexual violence within a trusted relationship can be profound. Because the abuse occurs within a relationship that is supposed to provide safety, survivors often experience a deep sense of betrayal in addition to the trauma itself.
Common effects include:
Anxiety or panic attacks
Depression
Shame and self-blame
Emotional numbness
Hypervigilance
Difficulty trusting others
Sleep disturbances and nightmares
Chronic pain
Dissociation
Fear of intimacy
Low sexual desire
Difficulty becoming aroused or reaching orgasm
Feeling disconnected during consensual intimacy
Some survivors also question whether they are "allowed" to call what happened rape because they loved—or still love—their partner. Loving someone does not erase the absence of consent.
Sexual Coercion or Pressure
Sexual coercion occurs when someone is pressured, manipulated, intimidated, or guilted into sexual activity they do not freely want. Unlike sexual assault involving physical force, sexual coercion often relies on emotional pressure, threats, manipulation, or an imbalance of power to obtain sex. While the tactics may be less obvious than physical violence, the emotional and psychological impact can be just as profound.
Healthy sexual experiences are built on freely given consent. If someone feels they have to say "yes" to avoid conflict, punishment, rejection, or harm, that is not true consent.
Many survivors of sexual coercion struggle to identify their experiences as traumatic because there may not have been physical force. They often question themselves by asking:
"I eventually said yes—does it still count?"
"Maybe I was overreacting."
"They never physically forced me."
"I could have left."
"I didn't want to, but I gave in."
These questions are incredibly common. The reality is that consent obtained through pressure, fear, manipulation, or coercion is not freely given consent.
What Does Sexual Coercion Look Like?
Sexual coercion can happen in dating relationships, marriages, friendships, casual relationships, workplaces, or situations where one person has more power or influence than the other.
Examples include:
Repeatedly asking for sex after someone has already said "no."
Guilt-tripping someone into sexual activity.
Threatening to end the relationship if they refuse sex.
Saying things like, "If you loved me, you would."
Threatening to cheat or find someone else.
Making someone feel responsible for another person's sexual needs.
Using anger, intimidation, or emotional outbursts to pressure someone into sex.
Pressuring someone while they are intoxicated or emotionally vulnerable.
Wearing someone down until they finally give in.
Using financial dependence, immigration status, housing, or other forms of control to obtain sex.
Sometimes coercion is subtle and happens gradually over months or years. Survivors may not recognize the pattern until much later because the pressure became normalized within the relationship.
Understanding Consent
Consent is not simply the absence of "no."
True consent is:
Freely given
Enthusiastic
Informed
Ongoing
Reversible at any time
A person can change their mind at any point, even after sexual activity has already begun.
Someone who agrees to sex because they are afraid of being yelled at, abandoned, manipulated, or punished is not making a completely free choice.
Healthy relationships respect a person's autonomy. A caring partner accepts "no" without punishment, guilt, manipulation, or retaliation.
Why Sexual Coercion Can Be So Confusing
Unlike physical assault, sexual coercion often occurs within otherwise loving or long-term relationships. Survivors may deeply care about their partner while also recognizing that they regularly felt pressured into unwanted sexual activity.
Many people minimize their experiences because they compare them to more physically violent forms of sexual assault. They may think:
"At least they didn't hit me."
"Other people have had it worse."
"I eventually agreed."
"It wasn't really rape."
These thoughts can make it difficult to recognize the emotional harm that coercion causes.
Trauma is not measured by how violent an experience appears from the outside. It is measured by how overwhelming, frightening, violating, or powerless the experience felt to the survivor.
The Emotional Impact of Sexual Coercion
Repeated sexual pressure can gradually change the way someone experiences intimacy and relationships.
Survivors may experience:
Anxiety before sexual activity.
Feeling obligated to have sex instead of wanting it.
Low sexual desire.
Difficulty identifying their own needs and boundaries.
Shame or self-blame.
Emotional numbness.
Resentment toward their partner.
Depression.
Loss of trust.
Fear of saying "no."
Dissociation during sex.
Pain during sexual activity.
Difficulty becoming aroused or reaching orgasm.
Erectile dysfunction related to anxiety or emotional distress.
Over time, sex may begin to feel like an obligation rather than a mutually enjoyable experience, making it increasingly difficult to experience desire, pleasure, or emotional connection.
Stealthing (Non-Consensual Condom Removal)
Stealthing, also known as non-consensual condom removal, occurs when a person intentionally removes a condom during sexual activity without their partner's knowledge or consent. It can also include intentionally damaging or sabotaging a condom before or during sex, such as poking holes in it or causing it to break on purpose.
Consent to sex with a condom is not the same as consent to sex without one.
When someone secretly removes or sabotages a condom, they change the conditions under which consent was given. This violates a person's ability to make an informed decision about their body, health, and reproductive choices. Because of this, many experts and legal systems recognize stealthing as a form of sexual violence or sexual assault.
Why Is Stealthing Harmful?
For many survivors, the harm extends far beyond the physical act itself.
Stealthing can leave someone feeling violated, betrayed, powerless, and unsafe. The person consented to one type of sexual activity but was unknowingly exposed to another. This loss of choice and bodily autonomy can have significant emotional and psychological consequences.
In addition to emotional trauma, stealthing may increase the risk of:
Sexually transmitted infections (STIs)
Unintended pregnancy
Anxiety and panic
Shame or self-blame
Loss of trust in future partners
Symptoms of post-traumatic stress disorder (PTSD)
Difficulty feeling safe during future sexual experiences
Many survivors describe the betrayal as one of the most painful parts of the experience. Trust was broken in a deeply personal way.
"But I Consented to Sex..."
One of the most common misconceptions about stealthing is that agreeing to sex automatically means agreeing to every aspect of the encounter.
It does not.
Consent is specific.
If someone agrees to have sex only if a condom is used, that condition is part of their consent. Removing the condom without permission changes the sexual activity entirely.
Think of consent as an agreement. If one person secretly changes the terms of that agreement without the other's knowledge, the original consent no longer applies.
Your consent matters—not only whether you agreed to have sex, but also how you agreed to have sex.
Why Survivors Often Question Themselves
Because awareness of stealthing is still growing, many survivors struggle to identify what happened.
You may find yourself thinking:
"Maybe I'm making too big of a deal out of this."
"I already agreed to sex."
"It happened so fast."
"I should have noticed."
"Maybe it was an accident."
These reactions are common.
Intentional condom removal without your knowledge or permission is fundamentally different from an accidental condom break. The defining feature of stealthing is deception. One person knowingly removes or sabotages protection without the other person's informed consent.
The Emotional Impact of Stealthing
Like other forms of sexual trauma, the emotional effects vary from person to person.
Some survivors experience:
Shock or disbelief
Anger
Anxiety
Panic attacks
Shame
Self-blame
Difficulty trusting partners
Hypervigilance
Fear during future sexual encounters
Avoidance of intimacy
Changes in sexual desire
Dissociation during sex
Others may not fully recognize the emotional impact until weeks, months, or even years later.
There is no "right" way to respond. Trauma affects everyone differently.
Drug- or Alcohol-Facilitated Sexual Assault
Drug- or alcohol-facilitated sexual assault occurs when someone is unable to freely consent to sexual activity because they have been voluntarily intoxicated, involuntarily drugged, or are otherwise incapacitated by alcohol or drugs. Some assaults involve substances that are secretly given to a person without their knowledge, while others occur when someone intentionally takes advantage of a person who is already too impaired to give informed consent.
Regardless of how the intoxication occurred, a person who is incapacitated cannot legally or ethically consent to sexual activity.
Many survivors blame themselves because they chose to drink alcohol or use recreational substances. However, choosing to drink is not the same as consenting to sex. Responsibility always lies with the person who chose to take advantage of someone who could not freely consent.
What Is Drug- or Alcohol-Facilitated Sexual Assault?
Drug- or alcohol-facilitated sexual assault can occur in many different ways.
Some examples include:
Secretly placing drugs into someone's drink without their knowledge.
Encouraging someone to consume excessive amounts of alcohol to reduce their ability to resist.
Taking advantage of someone who is heavily intoxicated or incapacitated.
Having sexual contact with someone who is asleep or unconscious after drinking or using drugs.
Continuing sexual activity after someone becomes too impaired to understand what is happening or communicate their wishes.
Although the media often focuses on "date rape drugs" such as GHB or Rohypnol, alcohol is actually one of the most common substances involved in drug- or alcohol-facilitated sexual assault. Many survivors were drinking voluntarily before the assault occurred.
Understanding Consent and Incapacitation
Consent requires the ability to make an informed, voluntary decision.
A person cannot provide meaningful consent if they are:
Unconscious.
Asleep.
Blacked out.
Severely intoxicated.
Unable to understand what is happening.
Unable to communicate their choices clearly.
Being intoxicated does not automatically mean someone lacks the capacity to consent. However, when a person's level of impairment prevents them from making informed decisions or communicating freely, they cannot legally or ethically consent to sexual activity.
The responsibility belongs to the person initiating sexual activity to ensure that consent is freely given.
Why Many Survivors Blame Themselves
Self-blame is one of the most common reactions after drug- or alcohol-facilitated sexual assault.
Survivors often think:
"I shouldn't have gone to that party."
"I drank too much."
"I put myself in that situation."
"Maybe I led them on."
"No one will believe me because I was drinking."
These thoughts are understandable, but they are not accurate.
Choosing to drink alcohol does not give another person permission to violate your body.
Just as leaving your car unlocked does not make theft acceptable, drinking alcohol does not make sexual assault acceptable. Responsibility always belongs to the person who chose to ignore or exploit another person's inability to consent.
Memory Gaps and Blackouts
One of the most confusing aspects of drug- or alcohol-facilitated sexual assault is that survivors may remember only parts of what happened—or nothing at all.
Alcohol and certain drugs can interfere with the brain's ability to form new memories. As a result, survivors may experience:
Partial memories.
Missing periods of time.
Feeling uncertain about what happened.
Fragments of memories that return later.
Confusion about whether the assault really occurred.
Trauma itself can also disrupt how memories are stored. The combination of intoxication and trauma often makes memory especially fragmented.
Not remembering every detail does not mean an assault did not happen.
The Emotional Impact
Survivors of drug- or alcohol-facilitated sexual assault often experience the same trauma symptoms seen after other forms of sexual violence, along with additional confusion related to memory loss and self-blame.
Common reactions include:
Shock.
Anxiety.
Panic attacks.
Depression.
Shame.
Guilt.
Hypervigilance.
Difficulty trusting others.
Nightmares.
Dissociation.
Fear of social situations.
Avoidance of alcohol or parties.
Changes in sexual desire.
Difficulty becoming aroused or reaching orgasm.
Erectile dysfunction related to trauma or anxiety.
Many survivors also struggle with uncertainty because they cannot remember every detail. This uncertainty can make it more difficult to seek support or report the assault.
Healing After Drug- or Alcohol-Facilitated Sexual Assault
Healing often begins by recognizing that you are not responsible for another person's decision to exploit your vulnerability.
Many survivors spend years replaying the night in their minds, wondering what they could have done differently. While these thoughts are common, recovery focuses on shifting responsibility back where it belongs.
Trauma-informed therapy can help survivors process traumatic memories, reduce shame and self-blame, rebuild trust in themselves, and reconnect with a sense of safety. Evidence-based treatments such as Eye Movement Desensitization and Reprocessing (EMDR), somatic therapies, and sex therapy have helped many survivors recover from the emotional effects of sexual violence.
Healing is possible—even if you don't remember every detail.
Your memory does not determine whether your experience was real.
Your body, your emotions, and your reactions deserve to be taken seriously.
Sexual Harassment
Sexual harassment is a form of unwanted sexual behavior that creates an intimidating, hostile, humiliating, or offensive environment. While some people think of sexual harassment as "just inappropriate comments," it can have profound emotional and psychological effects—especially when it is repeated, involves a power imbalance, or makes someone fear for their safety, job, education, or well-being.
Sexual harassment can occur anywhere, including workplaces, schools, colleges, healthcare settings, religious organizations, sports teams, military settings, public spaces, and online. It can happen between strangers, coworkers, classmates, supervisors, teachers, healthcare providers, family members, dating partners, or anyone in a position of authority or influence.
Not everyone who experiences sexual harassment develops trauma, but for many people—especially when the behavior is ongoing or threatening—it can become a traumatic experience.
What Is Sexual Harassment?
Sexual harassment includes unwanted sexual attention, comments, behaviors, or advances that interfere with a person's sense of safety, dignity, or ability to participate fully in work, school, or everyday life.
Sexual harassment may be:
Verbal
Physical
Nonverbal
Digital or online
It can happen once, but it more commonly occurs as a repeated pattern of behavior.
Examples of Sexual Harassment
Sexual harassment can take many forms, including:
Unwanted sexual comments or jokes.
Repeated requests for dates after someone has said no.
Sexually explicit text messages or emails.
Unwanted touching, hugging, or rubbing against someone's body.
Sexual gestures or sounds.
Comments about someone's body or appearance.
Sharing sexual images without consent.
Displaying sexually explicit material in the workplace or classroom.
Making sexual rumors about someone.
Catcalling.
Sending unwanted explicit photos.
Staring at someone's body in a way that feels intimidating or threatening.
Threatening someone's job, grades, or opportunities unless they comply with sexual requests.
Offering promotions, better grades, or other benefits in exchange for sexual favors.
The behavior does not have to involve physical contact to be harmful.
Quid Pro Quo vs. Hostile Work Environment
Sexual harassment is often divided into two broad categories.
Quid Pro Quo Harassment
"Quid pro quo" means "this for that."
This occurs when someone in a position of power makes employment, educational opportunities, promotions, grades, or other benefits contingent upon sexual cooperation.
Examples include:
A supervisor suggesting an employee will receive a promotion if they agree to a date.
A professor implying a student's grade depends on sexual attention.
A manager threatening termination after rejecting sexual advances.
Hostile Environment Harassment
A hostile environment develops when repeated sexual behavior creates an intimidating, offensive, or uncomfortable atmosphere that interferes with someone's ability to work, learn, or feel safe.
Examples include:
Repeated sexual jokes.
Persistent comments about someone's appearance.
Sexual conversations despite requests to stop.
Unwanted flirting.
Displaying sexually explicit materials.
Repeated inappropriate touching.
Sexual rumors or gossip.
One isolated comment may be inappropriate without meeting the legal definition of harassment, while repeated behaviors often create a hostile environment over time.
Why Sexual Harassment Can Be Traumatic
Many people underestimate the emotional impact of sexual harassment because it does not always involve physical assault.
However, repeated violations of personal boundaries can significantly affect a person's nervous system.
Survivors may begin to feel constantly on guard, anticipating the next inappropriate comment, unwanted touch, or uncomfortable interaction. Over time, this chronic stress can contribute to trauma symptoms.
For individuals who have previously experienced sexual assault or childhood sexual abuse, sexual harassment may also trigger memories of earlier trauma, making its effects even more intense.
The Emotional and Psychological Impact
People who experience ongoing sexual harassment may develop:
Anxiety.
Depression.
Chronic stress.
Hypervigilance.
Difficulty concentrating.
Sleep disturbances.
Panic attacks.
Low self-esteem.
Shame.
Anger.
Emotional exhaustion.
Burnout.
Fear of going to work or school.
Social withdrawal.
Difficulty trusting others.
Some survivors also experience changes in intimacy, including reduced sexual desire, increased anxiety around physical touch, or feeling emotionally disconnected from their bodies.
Common Myths About Sexual Harassment
Myth: "It was just a joke."
Fact: Humor does not erase the impact of unwanted sexual comments or behavior. What matters is how the behavior affects the person experiencing it.
Myth: "If they didn't touch you, it isn't harassment."
Fact: Sexual harassment does not require physical contact. Words, repeated comments, digital messages, gestures, and other unwanted behaviors can all be forms of harassment.
Myth: "You should have said something."
Fact: Many people stay silent because they fear retaliation, losing their job, damaging relationships, being labeled "difficult," or not being believed.
Myth: "You're overreacting."
Fact: Everyone has different boundaries and experiences. Feeling uncomfortable, unsafe, or intimidated by unwanted sexual behavior is a valid response.

Religious or Purity Culture Trauma
Religious or purity culture trauma occurs when religious teachings, spiritual beliefs, or cultural messages about sex, sexuality, gender, or the body create lasting fear, shame, guilt, or emotional distress. While faith and spirituality can be meaningful sources of comfort and healing for many people, harmful or rigid teachings about sexuality can sometimes leave individuals feeling disconnected from their bodies, fearful of intimacy, or ashamed of their natural sexual thoughts and desires.
Not everyone raised in a religious community experiences religious trauma. Many people have positive experiences with their faith. However, when religious beliefs are used to control, shame, manipulate, or instill fear around sexuality, they can have significant and lasting effects on mental health, relationships, and sexual well-being.
What Is Purity Culture?
Purity culture refers to belief systems that place a strong emphasis on sexual abstinence before marriage and often link a person's worth, morality, or spiritual value to their sexual behavior.
While many families and religions encourage abstinence as a personal or spiritual value, purity culture becomes harmful when it teaches that:
Sexual thoughts are sinful or dangerous.
Your worth depends on your sexual "purity."
Having sex before marriage permanently damages your value.
Sexual desire is shameful.
Men cannot control their sexual urges.
Women are responsible for preventing men from "stumbling."
Good people do not experience sexual desire.
Questioning sexual teachings is a sign of weak faith.
These messages can create deep internal conflict, particularly when they are reinforced throughout childhood and adolescence.
How Religious or Purity Culture Trauma Develops
Many people raised in strict religious environments learn to fear their own bodies and sexuality long before becoming sexually active.
They may receive messages such as:
"Sex is dirty."
"Good girls don't think about sex."
"Real men should always want sex."
"Your body tempts others to sin."
"Sex outside of marriage makes you damaged."
"If you have sexual thoughts, you're disappointing God."
Over time, these beliefs can become deeply ingrained and continue to affect someone well into adulthood, even if they no longer identify with the religion in which they were raised.
Some individuals also experience spiritual abuse, where religious beliefs are used to justify sexual abuse, discourage reporting abuse, pressure forgiveness before healing, or silence survivors. These experiences can intensify both psychological and spiritual trauma.
Common Effects of Religious or Purity Culture Trauma
Religious or purity culture trauma can affect nearly every aspect of a person's life.
Emotionally, survivors may experience:
Chronic shame.
Guilt.
Anxiety.
Depression.
Fear of making mistakes.
Perfectionism.
Difficulty trusting themselves.
Religious scrupulosity or obsessive fears about sin.
Sexually, survivors may experience:
Low sexual desire.
Difficulty becoming aroused.
Pain during sex.
Difficulty reaching orgasm.
Fear of intimacy.
Feeling "dirty" after consensual sex.
Anxiety before or during sexual activity.
Avoidance of physical affection.
Difficulty communicating sexual needs.
Feeling disconnected from pleasure.
Relationally, survivors may struggle with:
Fear of vulnerability.
Difficulty setting boundaries.
Fear of disappointing others.
Challenges discussing sex with a partner.
Difficulty reconciling faith and sexuality.
For some people, these symptoms closely resemble those seen after other forms of trauma because the nervous system has learned to associate sexuality with fear, danger, shame, or punishment rather than safety and connection.
Religious Trauma and Sexual Abuse
For some survivors, religious trauma and sexual abuse overlap.
Abuse may be committed by a trusted religious leader, family member, or member of a faith community. Survivors may also be told that reporting the abuse would dishonor their family, damage the church, or demonstrate a lack of forgiveness.
Others may have their abuse minimized by statements such as:
"Pray about it."
"God has already forgiven them."
"Don't cause division."
"You need to forgive and move on."
"Everything happens for a reason."
These responses can increase shame and make survivors feel isolated, unheard, or responsible for protecting the person who harmed them.
Military Sexual Trauma
Military Sexual Trauma (MST) refers to sexual assault, sexual harassment, or repeated unwanted sexual experiences that occur during military service. Unlike other forms of trauma, Military Sexual Trauma is not a diagnosis. Instead, it is a term used to describe experiences of sexual violence or harassment that happen while serving in the military, regardless of whether they occurred during training, deployment, active duty, or reserve service.
Military Sexual Trauma can affect service members of every rank, gender, sexual orientation, and military branch. Although women experience MST at higher rates, men also experience Military Sexual Trauma and often face additional barriers to reporting because of stigma, shame, and cultural expectations surrounding masculinity.
What Experiences Are Considered Military Sexual Trauma?
Military Sexual Trauma may include:
Sexual assault.
Attempted sexual assault.
Unwanted sexual touching.
Sexual coercion.
Sexual harassment.
Being pressured into sexual activity by someone in a position of authority.
Repeated sexual comments or advances that create a hostile environment.
Being forced to perform sexual acts.
Sexual violence during deployment or training.
Retaliation after reporting sexual misconduct.
Military Sexual Trauma can occur between peers, supervisors, commanding officers, healthcare providers, or others within the military environment. The person responsible may be someone the survivor knows, works with, or depends on professionally.
Why Military Sexual Trauma Can Be Especially Complex
Military Sexual Trauma often occurs within a culture built on trust, teamwork, discipline, and reliance on fellow service members.
When sexual violence occurs within that environment, survivors may experience multiple layers of betrayal. They are not only coping with the trauma itself but also with the loss of trust in the people and institution that were meant to provide protection and support.
Many survivors continue working or living alongside the person who harmed them. Others fear retaliation, damage to their military career, loss of promotions, social isolation, or being labeled as a troublemaker if they report what happened.
These unique circumstances can make Military Sexual Trauma especially difficult to process.
Barriers to Reporting
Many survivors choose not to report Military Sexual Trauma, and there are many understandable reasons why.
Some fear:
Retaliation.
Damage to their military career.
Being transferred instead of the person responsible.
Losing promotions or leadership opportunities.
Not being believed.
Being blamed for what happened.
Being viewed differently by fellow service members.
Isolation from their unit.
Re-traumatization during the reporting process.
These concerns are not signs of weakness. They reflect the complex realities many survivors face when deciding whether reporting feels safe.
The Effects of Military Sexual Trauma
Military Sexual Trauma can have lasting effects on emotional, physical, relational, and sexual well-being.
Common reactions include:
Post-traumatic stress disorder (PTSD).
Anxiety.
Depression.
Panic attacks.
Hypervigilance.
Nightmares.
Difficulty sleeping.
Emotional numbness.
Shame.
Guilt.
Anger.
Difficulty trusting others.
Dissociation.
Substance use.
Social withdrawal.
Military Sexual Trauma can also affect sexual health and relationships.
Some survivors experience:
Low sexual desire.
Fear of intimacy.
Difficulty becoming aroused.
Difficulty reaching orgasm.
Avoidance of physical touch.
Feeling emotionally disconnected during intimacy.
Because many military occupations involve high levels of stress and repeated exposure to danger, survivors may also be coping with combat-related trauma, making recovery more complex.
Military Sexual Trauma Is Not Limited by Gender
Although women experience Military Sexual Trauma at higher rates, thousands of men also experience sexual assault and harassment during military service.
Unfortunately, male survivors often face additional stigma because of harmful myths such as:
"Men can't be sexually assaulted."
"You should have fought back."
"Real men can defend themselves."
"Talking about it is a sign of weakness."
These myths prevent many survivors from seeking help.
Sexual assault can happen to anyone, regardless of gender, physical strength, or military training.
Human Trafficking and Sexual Exploitation
Human trafficking and sexual exploitation are among the most severe forms of interpersonal trauma. They involve the use of force, fraud, coercion, manipulation, or abuse of vulnerability to exploit another person for commercial sex or other forms of sexual gain. Survivors often experience repeated violations of their bodily autonomy, safety, trust, and basic human rights, leaving lasting emotional, psychological, physical, and relational effects.
A common misconception is that human trafficking always involves kidnapping or transporting someone across international borders. In reality, many survivors are trafficked within their own communities by someone they know and trust. Human trafficking can happen in large cities, small towns, affluent neighborhoods, rural communities, and online. It affects people of every age, gender, race, sexual orientation, and socioeconomic background.
What Is Human Trafficking?
Human trafficking is the recruitment, harboring, transportation, provision, or obtaining of a person through force, fraud, or coercion for the purpose of exploitation.
When the exploitation involves commercial sexual activity, it is referred to as sex trafficking.
Importantly, when the person being exploited is a minor, proof of force, fraud, or coercion is not required for the situation to be considered sex trafficking under U.S. law. Children cannot legally consent to commercial sexual exploitation.
What Is Sexual Exploitation?
Sexual exploitation occurs when someone is manipulated, pressured, deceived, or forced into sexual activity for another person's financial benefit, power, gratification, or control.
Sexual exploitation may include:
Commercial sexual exploitation.
Survival sex in exchange for basic needs such as food or housing.
Being pressured or manipulated into creating sexual content.
Being forced to engage in pornography.
Online exploitation through social media or messaging platforms.
Grooming for sexual exploitation.
Being coerced into exchanging sexual acts for money, drugs, shelter, or protection.
Being controlled by an intimate partner who profits from sexual activity.
Exploitation often occurs gradually. Many survivors do not initially recognize that they are being trafficked because the relationship began with affection, promises, gifts, or emotional support.
Grooming and Manipulation
Many traffickers use grooming rather than physical violence in the early stages.
Grooming is a process of building trust and emotional dependence before introducing exploitation.
A trafficker may:
Shower someone with attention or affection.
Offer financial support.
Promise love, safety, or a better future.
Isolate the person from friends and family.
Create emotional dependence.
Gradually increase control over decisions.
Use threats, intimidation, or violence once control has been established.
Because manipulation often develops slowly, survivors may later blame themselves for "not seeing it sooner."
The responsibility always belongs to the person who chose to exploit another human being.
Who Is at Risk?
Anyone can become a victim of trafficking or sexual exploitation.
However, traffickers often target individuals experiencing increased vulnerability, including those who may be:
Experiencing homelessness or housing instability.
Living in poverty.
Running away from home.
In foster care.
Experiencing family conflict or abuse.
Living with untreated mental health concerns.
Struggling with substance use.
Seeking love, belonging, or financial stability.
Socially isolated.
Experiencing previous trauma or abuse.
Being vulnerable does not cause trafficking. Traffickers intentionally exploit vulnerability for their own benefit.
The Impact of Human Trafficking and Sexual Exploitation
The effects of trafficking often extend far beyond the period of exploitation.
Many survivors experience:
Complex post-traumatic stress disorder (C-PTSD).
Anxiety.
Depression.
Dissociation.
Hypervigilance.
Chronic shame.
Guilt.
Emotional numbness.
Difficulty trusting others.
Sleep disturbances.
Substance use.
Self-harm.
Suicidal thoughts.
Chronic pain.
Medical complications.
Financial instability.
Trafficking can also profoundly affect sexual health and relationships.
Survivors may experience:
Low sexual desire.
Fear of intimacy.
Difficulty becoming aroused.
Difficulty reaching orgasm.
Feeling disconnected during consensual sexual activity.
Difficulty distinguishing healthy relationships from controlling ones.
Challenges setting boundaries.
Fear of vulnerability.
Many survivors also struggle with feelings of worthlessness or believe they are permanently "damaged." These beliefs are common trauma responses—not reflections of a person's value or future.
Why Leaving Isn't Simple
People often ask, "Why didn't they just leave?"
This question overlooks the reality of trafficking.
Many survivors remain in exploitative situations because they fear:
Violence against themselves or loved ones.
Retaliation.
Homelessness.
Financial instability.
Deportation.
Losing custody of their children.
Being arrested.
Not being believed.
Emotional abandonment.
Further abuse.
Trauma bonding, manipulation, isolation, and coercive control can create powerful psychological barriers that make leaving extremely difficult.
Remaining in a trafficking situation is never evidence that someone wanted or chose the abuse.
Image-Based Sexual Abuse
Image-based sexual abuse is the creation, sharing, distribution, or threat to distribute intimate or sexually explicit images or videos without a person's consent. While many people are familiar with the term "revenge porn," image-based sexual abuse is a much broader category that includes non-consensual sharing of intimate images, sexually explicit deepfake images and videos created with artificial intelligence (AI), hidden-camera recordings, sextortion, and digitally manipulated sexual content.
These experiences can have devastating emotional, psychological, social, and financial consequences. For many survivors, the trauma extends far beyond the image itself. The loss of privacy, control, and bodily autonomy can leave lasting effects that are similar to other forms of sexual violence.
What Is Image-Based Sexual Abuse?
Image-based sexual abuse occurs when intimate images or videos are created, shared, altered, or used without a person's knowledge or consent.
This may include:
Sharing private intimate photos or videos without permission.
Posting sexually explicit images online to humiliate or control someone.
Threatening to release intimate images unless someone complies with demands (sextortion).
Secretly recording someone during sexual activity.
Recording someone in private spaces, such as bathrooms or changing rooms, without their knowledge.
Creating sexually explicit deepfake images or videos using artificial intelligence (AI).
Digitally altering photographs to make it appear someone participated in sexual activity they never engaged in.
Distributing intimate images after a relationship ends.
Sharing explicit images in group chats, online forums, or social media without consent.
Whether the images are real or digitally created, the violation of consent and personal autonomy can have profound psychological effects.
What Is "Revenge Porn"?
"Revenge porn" is a commonly used term for the non-consensual sharing of intimate images, often by a current or former romantic partner.
However, many professionals now prefer the term non-consensual intimate image sharing or image-based sexual abuse because these terms better reflect the wide range of situations in which this abuse occurs.
Not all image-based sexual abuse is motivated by revenge. Images may be shared to embarrass, intimidate, control, extort, financially exploit, or simply humiliate another person.
Regardless of the motivation, sharing intimate images without consent is a violation of trust and bodily autonomy.
AI Deepfakes and Digital Sexual Exploitation
Advances in artificial intelligence have created new forms of image-based sexual abuse.
AI can now generate realistic-looking sexually explicit images or videos that falsely depict someone engaging in sexual activity, even if that person has never posed for or created explicit content.
These are commonly referred to as sexually explicit deepfakes.
Deepfake sexual images may be created using publicly available photographs from:
Social media accounts.
School or workplace websites.
Dating profiles.
Family photographs.
Professional headshots.
Other publicly accessible images.
Survivors often experience intense distress because the images can appear authentic, making it difficult for others to recognize that they were digitally created.
Even though the images are fake, the emotional impact is very real.
Survivors may experience humiliation, fear, damage to their reputation, workplace consequences, harassment, anxiety, and difficulty trusting others.
Sextortion
Sextortion occurs when someone threatens to share intimate images or videos unless the victim complies with demands.
These demands may include:
Sending additional intimate images.
Paying money.
Continuing a relationship.
Performing sexual acts.
Remaining silent about abuse.
Sextortion can occur between strangers, romantic partners, acquaintances, or people who initially met online.
The fear that intimate images could be shared publicly often leaves survivors feeling trapped, isolated, and powerless.
The Emotional Impact of Image-Based Sexual Abuse
Image-based sexual abuse can affect every aspect of a person's life.
Common emotional and psychological effects include:
Anxiety.
Depression.
Shame.
Humiliation.
Panic attacks.
Hypervigilance.
Difficulty sleeping.
Loss of trust.
Social withdrawal.
Fear of using social media.
Difficulty concentrating.
Emotional numbness.
Symptoms of post-traumatic stress disorder (PTSD).
Suicidal thoughts in severe cases.
Many survivors also experience fear that the images will continue resurfacing online, making it difficult to feel safe or move forward.
The ongoing uncertainty can create a sense that the trauma never truly ends.
Common Myths About Image-Based Sexual Abuse
Myth: "You shouldn't have taken the photo."
Fact: Choosing to create or share an intimate image with a trusted person does not give them permission to share it with anyone else. Consent to privately sharing an image is not consent for public distribution.
Myth: "It's not as serious because no physical contact occurred."
Fact: Image-based sexual abuse can have profound emotional, psychological, social, and financial consequences. Many survivors experience trauma symptoms similar to those seen after other forms of interpersonal violence.
Myth: "The AI image isn't real, so it shouldn't matter."
Fact: Sexually explicit deepfakes can damage reputations, careers, relationships, and mental health. Even when an image is digitally created, the violation of someone's identity, privacy, and dignity is real.
Online Sexual Abuse and Grooming
Online sexual abuse and grooming occur when someone uses digital technology to manipulate, exploit, coerce, or sexually abuse another person. Although these experiences happen through phones, computers, gaming platforms, social media, messaging apps, or other online spaces, the emotional and psychological effects are very real.
Many people mistakenly believe that abuse is "less serious" if there was no physical contact. However, survivors of online sexual abuse often experience the same feelings of fear, shame, betrayal, anxiety, and trauma as survivors of in-person abuse.
Online sexual abuse can affect both children and adults. It may involve strangers, but it can also be committed by classmates, dating partners, friends, family members, or someone the survivor has known for years.
What Is Online Grooming?
Online grooming is the process of building trust with someone in order to manipulate, exploit, or sexually abuse them.
Grooming often happens gradually. Rather than beginning with obvious abuse, the person responsible typically works to create a relationship built on trust, attention, affection, or emotional dependence before introducing sexual behavior.
Grooming may occur over days, months, or even years.
It is important to understand that grooming is intentional. The responsibility always belongs to the person choosing to manipulate another individual—not the survivor.
Common Grooming Tactics
Someone who is grooming another person may:
Give excessive compliments or attention.
Offer emotional support or affection.
Buy gifts or send money.
Encourage secrecy.
Gradually isolate the person from friends or family.
Test boundaries with sexual jokes or conversations.
Normalize increasingly sexual discussions.
Ask for private photos or videos.
Use guilt or emotional manipulation to maintain the relationship.
Threaten to end the relationship if requests are refused.
Threaten to share private images if someone tries to leave.
Many survivors later describe feeling that the relationship initially felt caring or supportive, making it difficult to recognize the manipulation until much later.
What Does Online Sexual Abuse Look Like?
Online sexual abuse can take many forms, including:
Sending unwanted sexual messages.
Pressuring someone to send intimate photos or videos.
Soliciting sexual images from a minor.
Sharing sexually explicit material without consent.
Sexual exploitation through live streaming.
Recording or distributing intimate content.
Sextortion.
Creating fake online identities to manipulate someone.
Using gaming platforms or social media to exploit children or vulnerable adults.
Coercing someone into performing sexual acts over video chat.
Threatening to release intimate images if demands are not met.
Technology continues to evolve, and so do the ways people exploit others online. Regardless of the method, the common thread is the violation of consent, safety, and personal autonomy.
Grooming Can Happen to Adults, Too
Although grooming is often discussed in relation to children, adults can also be groomed.
Adults experiencing loneliness, grief, financial hardship, relationship difficulties, or emotional vulnerability may be targeted by individuals who use affection, attention, promises of love, or financial support to build trust before becoming controlling or sexually exploitative.
This does not mean the survivor was "naive."
Manipulation is a deliberate strategy designed to lower defenses and create emotional dependence.
The Emotional Impact of Online Sexual Abuse
Online sexual abuse can have lasting effects on mental health and relationships.
Common reactions include:
Anxiety.
Depression.
Shame.
Fear.
Panic attacks.
Hypervigilance.
Social withdrawal.
Difficulty trusting others.
Sleep disturbances.
Emotional numbness.
Dissociation.
Symptoms of post-traumatic stress disorder (PTSD).
Difficulty forming new relationships.
Fear of using social media or online platforms.
Survivors may also experience changes in sexual functioning, including low sexual desire, fear of intimacy, difficulty becoming aroused, painful sex, erectile dysfunction, or difficulty reaching orgasm.
Many people continue to feel unsafe because digital content can remain online indefinitely or resurface unexpectedly.
Common Myths About Online Sexual Abuse
Myth: "It was only online."
Fact: Emotional and psychological trauma can occur regardless of whether abuse happened in person or through digital technology.
Myth: "I sent the pictures, so it's my fault."
Fact: Choosing to share an intimate image with someone you trusted does not give them permission to manipulate, exploit, threaten, or distribute that image.
Myth: "I should have known better."
Fact: Grooming is designed to build trust and lower defenses over time. Survivors are manipulated through carefully planned behaviors—not because they lack intelligence or judgment.
Myth: "Adults can't be groomed."
Fact: While children are especially vulnerable, adults can also be groomed through emotional manipulation, deception, financial dependence, or promises of love and support.
Reproductive Coercion
Reproductive coercion is a form of abuse in which one person attempts to control another person's reproductive choices, including whether they become pregnant, prevent pregnancy, continue a pregnancy, or end a pregnancy. It is a violation of bodily autonomy and reproductive freedom and often occurs alongside emotional abuse, intimate partner violence, sexual coercion, or physical abuse.
Unlike healthy relationships, where decisions about contraception and pregnancy are made together with mutual respect, reproductive coercion involves manipulation, deception, intimidation, or force to take away another person's ability to make informed decisions about their own body.
Many survivors do not realize they have experienced reproductive coercion because the behaviors are often disguised as expressions of love, concern, or a desire to start a family. However, when someone intentionally interferes with another person's reproductive choices without their consent, it is a form of abuse.
What Does Reproductive Coercion Look Like?
Reproductive coercion can take many different forms.
Examples include:
Hiding, destroying, or throwing away birth control pills.
Poking holes in condoms or intentionally damaging them.
Removing a condom during sex without consent (stealthing).
Refusing to use contraception after agreeing to do so.
Lying about having had a vasectomy.
Lying about using contraception.
Pressuring someone to become pregnant.
Pressuring someone not to become pregnant.
Threatening to end a relationship unless someone becomes pregnant.
Forcing or pressuring someone to continue a pregnancy against their wishes.
Forcing or pressuring someone to have an abortion against their wishes.
Preventing someone from accessing contraception or reproductive healthcare.
Monitoring menstrual cycles or medical appointments to maintain control.
Threatening violence or abandonment based on reproductive decisions.
The common thread is control. The goal is to take away another person's ability to freely decide what happens to their own body and future.
Reproductive Coercion Can Affect Anyone
Although reproductive coercion is most commonly discussed in the context of women, people of all genders can experience reproductive abuse.
For example, someone may:
Be deceived about contraception.
Be pressured into parenthood against their wishes.
Be manipulated into financial or emotional responsibility through deception.
Experience threats or coercion related to pregnancy or reproductive decisions.
Everyone has the right to make informed decisions about if, when, and how they become a parent.
Why Survivors Often Don't Recognize It
Reproductive coercion frequently develops within intimate relationships and may occur gradually over time.
Survivors often explain away controlling behaviors by thinking:
"They just really wanted a baby."
"They love me."
"Maybe I'm overreacting."
"They were only trying to protect me."
"I thought this was normal."
Because these behaviors often occur alongside affection or emotional attachment, many survivors struggle to identify them as abusive until much later.
Control is not the same as care.
Healthy relationships respect each person's right to make decisions about their own body and reproductive future.
The Emotional Impact of Reproductive Coercion
Reproductive coercion can have profound emotional, psychological, and relational effects.
Survivors may experience:
Anxiety.
Depression.
Shame.
Anger.
Grief.
Betrayal.
Loss of trust.
Hypervigilance.
Symptoms of post-traumatic stress disorder (PTSD).
Difficulty making future decisions.
Fear of intimacy.
Difficulty trusting future partners.
Changes in sexual desire or functioning.
Some survivors also experience complicated feelings about pregnancy, parenthood, infertility, abortion, or miscarriage as a result of the abuse.
There is no "right" emotional response. Every survivor's experience is unique.
Reproductive Coercion and Intimate Partner Violence
Reproductive coercion rarely occurs in isolation.
Research has shown that it often exists alongside other forms of abuse, including:
Emotional abuse.
Sexual coercion.
Physical violence.
Financial abuse.
Coercive control.
Stalking.
The more control an abusive partner seeks, the more likely reproductive decisions may become another way to maintain power within the relationship.

Does My Experience "Count" as Trauma?
One of the most common questions survivors ask is:
"Does what happened to me actually count as trauma?"
Many people minimize their experiences because they compare themselves to someone they believe had it "worse." They wonder if they are overreacting, being too sensitive, or making something out of nothing.
These thoughts are incredibly common.
The truth is that trauma is not measured by how dramatic an event looks from the outside. It is measured by how your mind, body, and nervous system responded to what happened.
An experience can be traumatic if it left you feeling overwhelmed, powerless, frightened, violated, trapped, or unable to cope—even if someone else might respond differently.
There is no "trauma threshold" that you must meet before your pain deserves to be taken seriously.
Trauma Is About Your Experience
Many people believe trauma only happens after extreme violence.
In reality, trauma can result from any experience that overwhelms your ability to cope and leaves lasting emotional, physical, psychological, or relational effects.
Two people can experience the exact same event and respond differently. One person may recover relatively quickly, while another develops symptoms of anxiety, post-traumatic stress disorder (PTSD), panic attacks, dissociation, or changes in relationships and sexual functioning.
Neither response is wrong.
Trauma is deeply personal.
Common Questions Survivors Ask
"I froze. Does it still count?"
Yes.
Freezing is one of the brain's automatic survival responses. During overwhelming danger, the nervous system may temporarily shut down movement or speech in an attempt to increase survival.
Freezing is not consent.
Many survivors are unable to scream, fight back, or even speak during an assault because their nervous system has automatically shifted into survival mode.
"I didn't fight back."
Many people don't.
Movies often portray survivors fighting or escaping, but research shows that involuntary responses such as freezing, complying, or dissociating are extremely common.
Your inability to resist does not mean you wanted what happened.
"I eventually said yes because I was scared."
Consent given out of fear is not freely given consent.
If you agreed because you feared violence, emotional abuse, abandonment, retaliation, manipulation, or continued pressure, your autonomy had already been compromised.
Healthy consent is freely given—not obtained through fear.
"We were dating."
Sexual assault can happen in dating relationships.
Being someone's partner does not eliminate the need for consent.
You have the right to say no in every relationship.
"We were married."
Marriage is not permanent consent.
Every person has the right to decide whether they want to engage in sexual activity, regardless of how long they have been together.
Marital rape and sexual coercion are recognized forms of sexual violence.
"I was drunk."
Choosing to drink alcohol is not the same as consenting to sex.
If someone intentionally took advantage of your inability to freely consent, responsibility belongs to them—not you.
"My body responded."
This is one of the most painful sources of shame for many survivors.
The human body can respond automatically to touch or sexual stimulation, even during assault.
Physical arousal is a biological reflex.
It is not evidence of consent.
It is not evidence that you wanted what happened.
It is not your fault.
"I don't remember everything."
Many survivors have fragmented memories.
Trauma changes how the brain stores information, and alcohol or drugs can further interfere with memory formation.
Not remembering every detail does not make your experience less real.
"It wasn't violent."
Many sexual assaults involve little or no physical violence.
Manipulation, coercion, intimidation, deception, emotional pressure, abuse of power, and taking advantage of someone's inability to consent can all result in profound trauma.
Violence is not required for trauma to occur.
"It happened years ago."
Trauma has no expiration date.
Many survivors begin experiencing symptoms months, years, or even decades later, particularly after entering a healthy relationship, becoming a parent, experiencing another stressful life event, or beginning therapy.
Healing can begin at any point.
You Don't Need Permission to Heal
One of the most damaging effects of trauma is self-doubt.
Many survivors spend years trying to determine whether what happened was "bad enough" before allowing themselves to seek support.
The better question is not:
"Was it bad enough?"
The better question is:
"How has it affected me?"
If your experiences have left you struggling with anxiety, shame, nightmares, panic, difficulty trusting others, fear of intimacy, low libido, painful sex, erectile dysfunction, dissociation, or feeling disconnected from yourself, those experiences deserve attention and care.
You do not have to prove your trauma.
You do not need someone else's experience to validate your own.
Your pain is not measured against another person's pain.
LGBTQIA+ Survivors: Special Considerations
Sexual trauma can happen to anyone, regardless of their sexual orientation or gender identity.
However, research consistently shows that lesbian, gay, bisexual, transgender, queer, intersex, asexual, and other LGBTQIA+ individuals experience sexual violence at higher rates than the general population. Despite this, many survivors face additional barriers when seeking safety, reporting the assault, or accessing supportive care.
If you are an LGBTQIA+ survivor, your experience matters.
You deserve to be believed, respected, and supported.
Higher Rates of Sexual Violence
LGBTQIA+ individuals experience disproportionately high rates of sexual violence across the lifespan.
This increased risk is influenced by many factors, including discrimination, hate crimes, social stigma, family rejection, homelessness among LGBTQIA+ youth, and violence within intimate relationships.
These experiences do not happen because of someone's identity.
They happen because perpetrators exploit vulnerability, power imbalances, and prejudice.
Fear of Not Being Believed
Many LGBTQIA+ survivors worry they won't be taken seriously.
They may fear that healthcare providers, law enforcement, family members, or even friends will dismiss their experience because of misconceptions about sexual orientation or gender identity.
Some survivors worry they will have to defend their identity before anyone will listen to what happened.
Everyone deserves to have their experience taken seriously.
Fear of Being "Outed"
For some survivors, reporting an assault or seeking medical care may carry another fear—the possibility of being "outed."
A person may worry that disclosing the assault could reveal their sexual orientation or gender identity to family members, employers, schools, religious communities, or others before they are ready.
This fear can prevent survivors from seeking the support they deserve.
Myths About Consent in LGBTQIA+ Relationships
Unfortunately, harmful myths still exist about sexual violence in LGBTQIA+ relationships.
Some people mistakenly believe:
Sexual assault only happens in heterosexual relationships.
Two people of the same gender cannot sexually assault one another.
Gender identity determines who can be a victim or perpetrator.
Sexual assault is less harmful in LGBTQIA+ relationships.
None of these beliefs are true.
Sexual assault is defined by the absence of consent—not by the gender, sexual orientation, or identity of the people involved.
Anyone can experience sexual violence.
Anyone can violate another person's consent.
Transgender and Nonbinary Survivors
Transgender and nonbinary individuals often face additional challenges after sexual trauma.
Some survivors report avoiding medical care because they fear discrimination or being misgendered.
Others worry that healthcare providers lack training in working with transgender patients or that they will have to educate their provider while coping with the effects of trauma.
Finding an affirming, trauma-informed provider can make a significant difference in the healing process.
Every survivor deserves healthcare where their identity is respected.
Finding Affirming Care
Healing is often easier when you don't have to explain or defend who you are.
When looking for a therapist or healthcare provider, it may be helpful to ask whether they have experience working with LGBTQIA+ clients and whether they provide gender-affirming, trauma-informed care.
An affirming provider recognizes that your identity is not the problem.
The trauma is.
Your care should be centered on healing—not on questioning or challenging who you are.
Male Survivors: Special Considerations
Sexual trauma can happen to anyone, including men.
Although sexual violence against men is more common than many people realize, male survivors are often overlooked in conversations about sexual assault. Harmful stereotypes about masculinity can make it difficult for men to recognize what happened to them, talk about their experiences, or seek help.
If you are a man who has experienced sexual trauma, you are not alone.
Your experience is real.
And you deserve support.
Sexual Trauma Happens to Men
Men experience sexual assault in many different situations.
This can include:
Childhood sexual abuse.
Sexual assault by a stranger.
Assault by a friend, family member, or partner.
Military sexual trauma.
Sexual violence in prisons or detention facilities.
Drug- or alcohol-facilitated sexual assault.
Sexual coercion or pressure.
Sexual trauma can affect men of every age, sexual orientation, race, and background.
Harmful Myths About Male Survivors
Many male survivors struggle because of harmful myths they have heard throughout their lives.
These myths include:
"Men always want sex."
"A real man could fight someone off."
"If you had an erection, you must have wanted it."
"Only gay men are sexually assaulted."
"Men can't be victims."
None of these statements are true.
Consent is not determined by gender.
A physical response is not the same as consent.
And being unable to fight back is a common survival response—not a sign of weakness.
Shame Can Keep Men Silent
Many men grow up believing they should always be strong, in control, and able to protect themselves.
After sexual trauma, these beliefs can create intense feelings of shame.
Some men wonder:
"Why didn't I stop it?"
"Does this make me weak?"
"What does this say about me?"
"Will anyone believe me?"
These thoughts are common, but they are based on myths—not facts.
Surviving trauma says nothing about your strength, masculinity, or worth.
Sexual Orientation Does Not Cause Sexual Assault
Some male survivors question their sexual orientation after being assaulted, especially if the perpetrator was another man.
Others worry that people will assume they are gay because they were assaulted.
Sexual assault is an act of violence, power, and control.
It is not determined by the survivor's sexual orientation, and it does not change who you are.
Likewise, gay, bisexual, and queer men can also experience sexual assault. Their experiences are just as real and deserving of support.
Trauma Can Affect Sexual Functioning
Many men experience changes in their sexual health after trauma.
These changes may include:
Low sexual desire.
Difficulty reaching orgasm.
Avoiding intimacy.
Feeling emotionally disconnected during sex.
Hypersexuality as a coping strategy.
These are common trauma responses.
They are not personal failures, and they do not mean you are "less of a man."
Why Many Men Don't Report
Male survivors are less likely to report sexual assault than female survivors.
Common reasons include:
Fear of not being believed.
Shame or embarrassment.
Fear of being judged.
Concerns about masculinity.
Fear of being blamed.
Not recognizing the experience as sexual assault.
Believing they should "just get over it."
These barriers can leave men feeling isolated, but they are not alone.
More men are speaking openly about sexual trauma than ever before, helping reduce stigma and encourage others to seek support.
Sex Workers: Special Considerations
Sex workers can and do experience sexual trauma.
One of the most harmful myths about sexual violence is the belief that someone cannot be sexually assaulted if they have agreed to sexual activity in exchange for money, goods, or services.
This is not true.
Consent must be present for every sexual act, every time.
A person's occupation never removes their right to bodily autonomy, safety, or consent.
Consent Can Be Withdrawn
Consent is not an all-or-nothing agreement.
Agreeing to one activity does not mean agreeing to everything.
Consent can be withdrawn at any time, regardless of whether money has been exchanged.
For example, sexual assault can occur if:
A client forces an act that was never agreed to.
A condom is removed without consent.
A client ignores a request to stop.
Physical force, threats, or intimidation are used.
Someone is too intoxicated or impaired to give consent.
Boundaries that were clearly established are violated.
Every person has the right to decide what happens to their body.
Barriers to Reporting
Many sex workers choose not to report sexual violence because they fear they will not be believed or will be blamed for what happened.
Some worry about:
Being judged because of their occupation.
Criminalization or legal consequences.
Losing income.
Experiencing discrimination.
Being dismissed by healthcare providers or law enforcement.
Having previous experiences of not being believed.
These barriers can leave survivors feeling isolated and unsupported.
No one should have to choose between their safety and the fear of being judged.
Trauma Is Trauma
The emotional and physical effects of sexual trauma are not determined by someone's occupation.
Sex workers may experience the same trauma responses as any other survivor, including:
Anxiety.
Depression.
PTSD.
Dissociation.
Shame.
Hypervigilance.
Nightmares.
Changes in sexual desire.
Difficulty trusting others.
Relationship challenges.
These reactions are normal responses to traumatic experiences.
Compassionate, Trauma-Informed Care Matters
Every survivor deserves healthcare and mental health treatment that is respectful, nonjudgmental, and trauma-informed.
Healing is most likely to happen when survivors feel safe enough to speak openly without fear of being criticized or blamed.
A trauma-informed therapist focuses on what happened to you—not on judging your occupation or personal choices.
Everyone deserves care that is rooted in dignity, respect, and compassion.
Survivors With Disabilities: Special Considerations
People with disabilities experience sexual violence at significantly higher rates than the general population. Yet despite this increased risk, they often face additional barriers to reporting abuse, accessing services, and receiving appropriate support.
Disabilities can include physical, intellectual, developmental, sensory, cognitive, or psychiatric disabilities.
No matter the type of disability, every person has the right to bodily autonomy, consent, safety, and respectful care.
Increased Risk of Sexual Violence
People with disabilities may be at greater risk for sexual violence for many reasons, including:
Dependence on others for personal care.
Social isolation.
Communication barriers.
Limited access to sexual health education.
Being targeted by perpetrators who believe they are less likely to be believed.
Greater dependence on caregivers, family members, or authority figures.
Sexual violence against people with disabilities is never caused by the disability itself.
It is the result of someone choosing to exploit vulnerability or a position of power.
Abuse by Trusted Individuals
Unlike the common image of a stranger assaulting someone, many survivors with disabilities know the person who harmed them.
The perpetrator may be:
A family member.
A Caregiver.
A Personal care attendant.
A healthcare provider.
A Transportation provider.
A Teacher.
A Friend.
A Romantic partner.
When someone depends on another person for daily care or support, reporting abuse can feel especially difficult.
Survivors may fear losing essential care, housing, transportation, or financial support if they disclose what happened.
Barriers to Reporting
Many survivors with disabilities face unique obstacles when trying to seek help.
These may include:
Fear of not being believed.
Difficulty accessing transportation.
Communication challenges.
Limited availability of accessible services.
Dependence on the person causing harm.
Fear of retaliation.
Previous experiences of discrimination.
Concerns that others will make decisions for them.
These barriers can make survivors feel trapped or alone.
No one should have to face those challenges while trying to heal.
Everyone Deserves to Be Believed
Unfortunately, some survivors with disabilities have been told that they misunderstood what happened or that their experiences are less credible because of their disability.
These assumptions are harmful.
People with disabilities deserve to have their experiences taken seriously.
Every survivor deserves to be listened to with respect, compassion, and dignity.
Accessible, Trauma-Informed Care Matters
Healing should be accessible to everyone.
Trauma-informed providers work to create environments where survivors feel physically and emotionally safe.
This may include:
Accessible office spaces.
Clear communication.
Extra time during appointments.
Alternative communication methods when needed.
Respect for autonomy and decision-making.
Collaboration with the survivor about what feels safe.
Every person deserves healthcare and therapy that respects both their identity and their individual needs.

Part 2: How Trauma Changes the Brain and Body
The Survival Response
When people think about trauma, they often wonder why survivors reacted the way they did.
Questions like:
"Why didn't I fight back?"
"Why couldn't I scream?"
"Why did I freeze?"
"Why did I go along with it?"
"Why did I stay?"
These are some of the most common questions survivors ask themselves—and unfortunately, they are also questions that others often ask after a traumatic event.
The answer lies in how the brain and nervous system are designed to keep us alive.
When the brain detects danger, it acts much faster than our conscious thinking mind. Before you have time to logically decide what to do, your nervous system automatically chooses the survival response it believes gives you the best chance of surviving the situation.
These responses are not conscious choices.
They are automatic, biological survival mechanisms that have evolved over thousands of years to protect us from harm.
Although many people have heard of "fight or flight," researchers now recognize four common trauma responses:
Fight
Flight
Freeze
Fawn
Every response has the same goal:
Survival.
There is no "right" or "wrong" survival response.
Your nervous system does not choose the response that looks the bravest—it chooses the one it believes is most likely to keep you alive.
Fight
The fight response occurs when the brain believes confronting the threat offers the best chance of survival.
During a fight response, the body prepares to defend itself by releasing stress hormones such as adrenaline.
Someone experiencing a fight response may:
Yell or scream.
Push, hit, kick, or physically resist.
Set firm verbal boundaries.
Become angry or aggressive.
Attempt to escape by fighting back.
Afterward, survivors who fought back may wonder if they could have done more.
The answer is almost always no.
Your nervous system responded with the tools it had available in that moment.
Flight
The flight response occurs when the brain decides the safest option is to escape.
Someone experiencing a flight response may:
Run away.
Hide.
Leave the situation quickly.
Avoid the person afterward.
Become extremely restless or anxious.
Sometimes escape is not physically possible.
When the brain recognizes there is no safe way to flee, it may automatically shift into another survival response, such as freeze or fawn.
This is why someone who initially tried to leave may suddenly become unable to move or speak.
Freeze
The freeze response is one of the most misunderstood trauma responses.
During a freeze response, the nervous system temporarily immobilizes the body.
A survivor may:
Be unable to move.
Be unable to speak.
Feel physically stuck.
Feel detached from what is happening.
Experience a racing mind while their body remains still.
Many survivors later ask:
"Why didn't I do anything?"
The answer is simple:
Because your brain did something.
It froze.
Freeze is not weakness.
It is not consent.
It is not choosing to "let it happen."
It is an involuntary survival response controlled by the nervous system.
Researchers often refer to this response as tonic immobility, and studies have found that it is extremely common during sexual assault.
Understanding the freeze response helps many survivors release years of unnecessary shame and self-blame.
Fawn
The fawn response occurs when the nervous system believes the safest way to survive is by keeping the threatening person calm or satisfied.
Someone experiencing a fawn response may:
Agree with the other person.
Try to keep the peace.
Apologize.
Laugh nervously.
Comply with demands.
Focus on making the other person happy.
Prioritize the other person's emotions over their own safety.
Afterward, survivors often wonder:
"Why did I go along with it?"
"Why was I nice to them?"
"Why didn't I just leave?"
The fawn response is not consent.
It is a survival strategy.
For many people—especially those who experienced childhood abuse, neglect, domestic violence, or controlling relationships—the nervous system has learned that compliance sometimes reduces danger.
In those moments, pleasing the other person may feel like the safest available option.
Why Different People Respond Differently
There is no single "correct" trauma response.
Your nervous system considers many factors before automatically choosing a survival strategy, including:
Whether escape is possible.
The size and strength of the threat.
Previous traumatic experiences.
Your relationship with the person.
Your environment.
Your past learning about safety and danger.
Two people can experience the same event and have completely different survival responses.
Neither response is more valid than the other.
Can Someone Experience More Than One Response?
Absolutely.
Trauma responses often shift throughout an event.
For example, someone might:
Initially try to fight.
Then attempt to run.
Freeze when escape becomes impossible.
Finally comply in an attempt to survive.
This is one of the reasons survivors sometimes feel confused about their own behavior.
Your nervous system is constantly reassessing danger and changing strategies as the situation unfolds.
The Survival Response
When people think about trauma, they often wonder why survivors reacted the way they did.
Questions like:
"Why didn't I fight back?"
"Why couldn't I scream?"
"Why did I freeze?"
"Why did I go along with it?"
"Why did I stay?"
These are some of the most common questions survivors ask themselves—and unfortunately, they are also questions that others often ask after a traumatic event.
The answer lies in how the brain and nervous system are designed to keep us alive.
When the brain detects danger, it acts much faster than our conscious thinking mind. Before you have time to logically decide what to do, your nervous system automatically chooses the survival response it believes gives you the best chance of surviving the situation.
These responses are not conscious choices.
They are automatic, biological survival mechanisms that have evolved over thousands of years to protect us from harm.
Although many people have heard of "fight or flight," researchers now recognize four common trauma responses:
Fight
Flight
Freeze
Fawn
Every response has the same goal:
Survival.
There is no "right" or "wrong" survival response.
Your nervous system does not choose the response that looks the bravest—it chooses the one it believes is most likely to keep you alive.
Fight
The fight response occurs when the brain believes confronting the threat offers the best chance of survival.
During a fight response, the body prepares to defend itself by releasing stress hormones such as adrenaline.
Someone experiencing a fight response may:
Yell or scream.
Push, hit, kick, or physically resist.
Set firm verbal boundaries.
Become angry or aggressive.
Attempt to escape by fighting back.
Afterward, survivors who fought back may wonder if they could have done more.
The answer is almost always no.
Your nervous system responded with the tools it had available in that moment.
Flight
The flight response occurs when the brain decides the safest option is to escape.
Someone experiencing a flight response may:
Run away.
Hide.
Leave the situation quickly.
Avoid the person afterward.
Become extremely restless or anxious.
Sometimes escape is not physically possible.
When the brain recognizes there is no safe way to flee, it may automatically shift into another survival response, such as freeze or fawn.
This is why someone who initially tried to leave may suddenly become unable to move or speak.
Freeze
The freeze response is one of the most misunderstood trauma responses.
During a freeze response, the nervous system temporarily immobilizes the body.
A survivor may:
Be unable to move.
Be unable to speak.
Feel physically stuck.
Feel detached from what is happening.
Experience a racing mind while their body remains still.
Many survivors later ask:
"Why didn't I do anything?"
The answer is simple:
Because your brain did something.
It froze.
Freeze is not weakness.
It is not consent.
It is not choosing to "let it happen."
It is an involuntary survival response controlled by the nervous system.
Researchers often refer to this response as tonic immobility, and studies have found that it is extremely common during sexual assault.
Understanding the freeze response helps many survivors release years of unnecessary shame and self-blame.
Fawn
The fawn response occurs when the nervous system believes the safest way to survive is by keeping the threatening person calm or satisfied.
Someone experiencing a fawn response may:
Agree with the other person.
Try to keep the peace.
Apologize.
Laugh nervously.
Comply with demands.
Focus on making the other person happy.
Prioritize the other person's emotions over their own safety.
Afterward, survivors often wonder:
"Why did I go along with it?"
"Why was I nice to them?"
"Why didn't I just leave?"
The fawn response is not consent.
It is a survival strategy.
For many people—especially those who experienced childhood abuse, neglect, domestic violence, or controlling relationships—the nervous system has learned that compliance sometimes reduces danger.
In those moments, pleasing the other person may feel like the safest available option.
Why Different People Respond Differently
There is no single "correct" trauma response.
Your nervous system considers many factors before automatically choosing a survival strategy, including:
Whether escape is possible.
The size and strength of the threat.
Previous traumatic experiences.
Your relationship with the person.
Your environment.
Your past learning about safety and danger.
Two people can experience the same event and have completely different survival responses.
Neither response is more valid than the other.
Can Someone Experience More Than One Response?
Absolutely.
Trauma responses often shift throughout an event.
For example, someone might:
Initially try to fight.
Then attempt to run.
Freeze when escape becomes impossible.
Finally comply in an attempt to survive.
This is one of the reasons survivors sometimes feel confused about their own behavior.
Your nervous system is constantly reassessing danger and changing strategies as the situation unfolds.

The Brain on Trauma
One of the most important things to understand about sexual trauma is this:
Trauma changes the brain—but the brain can heal.
For many survivors, learning how trauma affects the brain is incredibly validating. Instead of asking, "What's wrong with me?" they begin asking a different question:
"What happened to my brain and nervous system?"
This shift can reduce years of shame and self-blame.
Your reactions after trauma are not signs of weakness or failure. They are the result of a brain that adapted to survive an overwhelming experience.
The good news is that the brain is capable of healing. Thanks to a process called neuroplasticity, the brain can form new neural pathways throughout life. With time, safety, and evidence-based treatment, many trauma-related changes can improve significantly.
How the Brain Responds to Trauma
When your brain senses danger, it shifts into survival mode.
Instead of focusing on learning, planning, or problem-solving, the brain prioritizes one goal:
Stay alive.
To do this, several areas of the brain begin working differently.
Although these changes are incredibly helpful during a dangerous situation, they can become problematic when the brain continues responding as though danger is still present long after the trauma has ended.
Let's look at the four major brain regions involved in trauma.
The Amygdala: The Brain's Alarm System
The amygdala is a small almond-shaped structure deep within the brain that acts as your internal alarm system.
Its job is to constantly scan for danger.
When it detects a threat, it rapidly activates your body's stress response by releasing stress hormones and preparing you to fight, flee, freeze, or fawn.
After sexual trauma, the amygdala often becomes overactive.
Instead of only responding to genuine danger, it may begin reacting to reminders of the trauma—even when you are objectively safe.
For example, your amygdala may respond to:
A particular smell.
A certain voice.
Physical touch.
A medical examination.
A sexual situation.
A crowded room.
Someone standing too close.
A specific song.
Certain clothing.
A relationship conflict.
Because the amygdala responds before your thinking brain has time to evaluate the situation, survivors often experience fear before they understand why.
This is why someone may logically know they are safe while their body still reacts as though danger is happening.
The Hippocampus: The Memory Center
The hippocampus helps organize memories by placing them into context.
It answers questions such as:
When did this happen?
Where did it happen?
Is it happening now or is it over?
Trauma can interfere with how the hippocampus stores memories.
Instead of being filed away as a completed event from the past, traumatic memories may remain fragmented or feel as though they are happening in the present.
This helps explain why survivors may experience:
Flashbacks.
Intrusive memories.
Nightmares.
Memory gaps.
Difficulty remembering parts of the trauma.
Feeling like the trauma is happening all over again.
Many survivors worry because they cannot remember every detail of what happened.
This is actually a common trauma response.
Traumatic memories are often stored differently than ordinary memories.
The Prefrontal Cortex: The Thinking Brain
The prefrontal cortex is responsible for reasoning, planning, decision-making, emotional regulation, and impulse control.
Think of it as the brain's "CEO."
During trauma, the prefrontal cortex becomes less active while the survival areas of the brain take over.
This is why many survivors report:
Difficulty thinking clearly.
Trouble making decisions.
Feeling mentally "foggy."
Difficulty concentrating.
Trouble finding words.
Feeling disconnected from themselves.
Your brain temporarily shifts resources away from logical thinking because survival is more important than analysis.
Unfortunately, some people continue experiencing these symptoms long after the traumatic event has ended because their nervous system remains stuck in survival mode.
The Anterior Cingulate Cortex (ACC): The Emotional Regulation Center
The anterior cingulate cortex (ACC) helps regulate emotions, shift attention, solve problems, and calm the brain after stress.
Following trauma, this area may become underactive, making it more difficult to regulate emotions and return to a calm state after becoming upset.
Survivors may notice:
Emotional overwhelm.
Feeling "stuck" in emotions.
Difficulty calming down after conflict.
Trouble shifting attention away from distressing thoughts.
Increased anxiety.
Difficulty tolerating uncertainty.
When the ACC is not functioning efficiently, even relatively small stressors can feel overwhelming because the brain struggles to transition back into a state of safety.
The Insula: The Body Awareness Center
The insula helps you notice and interpret signals coming from inside your body.
It allows you to recognize sensations such as:
Hunger.
Pain.
Muscle tension.
Heart rate.
Breathing.
Sexual arousal.
Emotional "gut feelings."
After trauma, the insula may become dysregulated.
Some survivors become extremely aware of bodily sensations, while others feel disconnected from their bodies altogether.
This may contribute to:
Dissociation.
Feeling numb.
Feeling disconnected during intimacy.
Difficulty recognizing emotions.
Chronic pain.
Panic attacks.
Fear of physical touch.
For many survivors of sexual trauma, reconnecting safely with the body becomes an important part of healing.
Trauma Affects the Whole Nervous System
Trauma is not "just in your head."
It affects your entire nervous system.
This is why survivors often experience symptoms that seem unrelated to the original trauma, including:
Muscle tension.
Chronic pain.
Digestive problems.
Sleep disturbances.
Fatigue.
Headaches.
Panic attacks.
Startle responses.
Sexual dysfunction.
Difficulty reaching orgasm.
These symptoms are real physiological responses—not signs that someone is "overreacting."
The Brain Can Heal
Perhaps the most hopeful finding in trauma research is that the brain remains capable of change throughout life.
This ability is called neuroplasticity.
Neuroplasticity means the brain can build new neural pathways based on repeated experiences of safety, connection, and healing.
Evidence-based treatments such as Eye Movement Desensitization and Reprocessing (EMDR), somatic therapies, mindfulness practices, and other trauma-informed approaches can help reduce trauma symptoms by helping the brain process traumatic memories more adaptively.
As healing occurs, many survivors notice:
Fewer flashbacks.
Less anxiety.
Better emotional regulation.
Improved concentration.
More restful sleep.
Greater ability to experience intimacy.
Reduced fear.
Increased feelings of safety.
More confidence in relationships.
Healing does not erase the past.
It changes how the brain stores and responds to it.

The Window of Tolerance
One of the most helpful concepts for understanding trauma is the Window of Tolerance.
Developed by psychiatrist Dr. Dan Siegel, the Window of Tolerance describes the zone in which your brain and nervous system are able to function at their best. When you're within your window, you can think clearly, regulate your emotions, solve problems, connect with others, and respond to stress in healthy ways.
Everyone has a Window of Tolerance.
Some people naturally have a wider window, while others have a narrower one due to genetics, life experiences, chronic stress, or trauma.
After sexual trauma, many survivors find that their Window of Tolerance becomes much smaller. Things that once felt manageable may suddenly feel overwhelming or completely shutting down.
This is not because you are weak.
It is because your nervous system has become more sensitive after experiencing danger.
What Happens Inside Your Window?
When you're within your Window of Tolerance, your nervous system feels relatively balanced.
You are more likely to:
Feel calm and grounded.
Think clearly.
Make decisions.
Regulate your emotions.
Solve problems.
Feel connected to yourself and others.
Learn new information.
Be present during conversations.
Experience intimacy and pleasure more comfortably.
Recover from stress more quickly.
This doesn't mean you never feel anxious, sad, or frustrated.
It simply means your nervous system can experience these emotions without becoming overwhelmed.
Hyperarousal: When You Go Above Your Window
When stress becomes too intense, your nervous system may move above your Window of Tolerance into a state called hyperarousal.
Hyperarousal is your body's "high alert" mode.
It is driven by the sympathetic nervous system, which prepares you to fight or flee from danger.
Common signs of hyperarousal include:
Anxiety.
Panic attacks.
Racing thoughts.
Hypervigilance.
Irritability.
Anger.
Feeling "on edge."
Difficulty sleeping.
Increased heart rate.
Muscle tension.
Startling easily.
Feeling unable to relax.
For survivors of sexual trauma, reminders of the trauma may push the nervous system into hyperarousal, even when there is no actual danger in the present moment.
Your body reacts as though the threat is happening again.
Hypoarousal: When You Fall Below Your Window
At other times, the nervous system may move below the Window of Tolerance into a state called hypoarousal.
Instead of becoming activated, the body begins to shut down in an attempt to conserve energy and survive overwhelming stress.
Common signs of hypoarousal include:
Emotional numbness.
Feeling disconnected.
Dissociation.
Fatigue.
Difficulty concentrating.
Feeling "spaced out."
Feeling detached from your body.
Low motivation.
Feeling emotionally flat.
Difficulty speaking.
Wanting to withdraw from others.
Many survivors mistakenly believe they are "lazy" or "broken" when they are actually experiencing a protective nervous system response.
Hypoarousal is often associated with the freeze response discussed in the previous chapter.
Why Trauma Shrinks the Window of Tolerance
After trauma, the brain becomes more sensitive to potential danger.
An overactive amygdala, changes in the hippocampus, and reduced activity in the prefrontal cortex make it easier for the nervous system to leave the Window of Tolerance.
This means everyday experiences may suddenly trigger intense reactions.
For example:
A partner touching your shoulder.
Hearing a raised voice.
Receiving criticism.
Visiting a doctor's office.
Smelling a familiar cologne or perfume.
Watching a movie with sexual violence.
Experiencing conflict in a relationship.
Although these situations may not be dangerous, your brain may interpret them as reminders of past trauma.
This is why survivors often say,
"I know I'm safe, but my body doesn't believe it."
The Window of Tolerance and Sexual Intimacy
For many survivors, intimacy itself can become a trigger.
A loving touch, kissing, nudity, or consensual sexual activity may activate memories stored within the nervous system.
Some survivors move into hyperarousal and experience:
Panic.
Fear.
Muscle tension.
Racing thoughts.
Difficulty relaxing.
Pain during sex.
Others move into hypoarousal and may experience:
Emotional numbness.
Dissociation.
Feeling disconnected.
Difficulty experiencing pleasure.
Difficulty becoming aroused.
Feeling absent during intimacy.
Neither response means something is wrong with you.
Both are signs that your nervous system is trying to protect you.
Can the Window of Tolerance Grow?
Yes.
One of the goals of trauma treatment is to gradually expand the Window of Tolerance.
As the brain and nervous system begin recognizing that the danger has passed, survivors often find they can tolerate a wider range of emotions without becoming overwhelmed or shutting down.
Evidence-based treatments such as Eye Movement Desensitization and Reprocessing (EMDR), somatic therapies, mindfulness practices, grounding exercises, breathing techniques, and trauma-informed psychotherapy can all help increase nervous system flexibility.
Over time, many survivors notice that they:
Recover from stress more quickly.
Feel calmer.
Experience fewer panic attacks.
Feel more present.
Regulate emotions more easily.
Sleep better.
Feel safer in relationships.
Enjoy intimacy again.
Experience greater confidence and resilience.
Healing does not mean you will never become overwhelmed.
It means your nervous system becomes better able to return to a place of safety.
Learning to Recognize Your Window
An important part of recovery is learning to notice where your nervous system is throughout the day.
Ask yourself:
Am I feeling calm and connected?
Am I becoming anxious or overwhelmed?
Am I shutting down or feeling disconnected?
What helped me feel safe today?
What pushed me outside my Window of Tolerance?
The more familiar you become with your nervous system, the easier it becomes to recognize your needs and use skills that help you return to a place of balance.
Recovery isn't about never leaving your Window of Tolerance.
It's about learning how to recognize when you've left it—and knowing that you can find your way back.
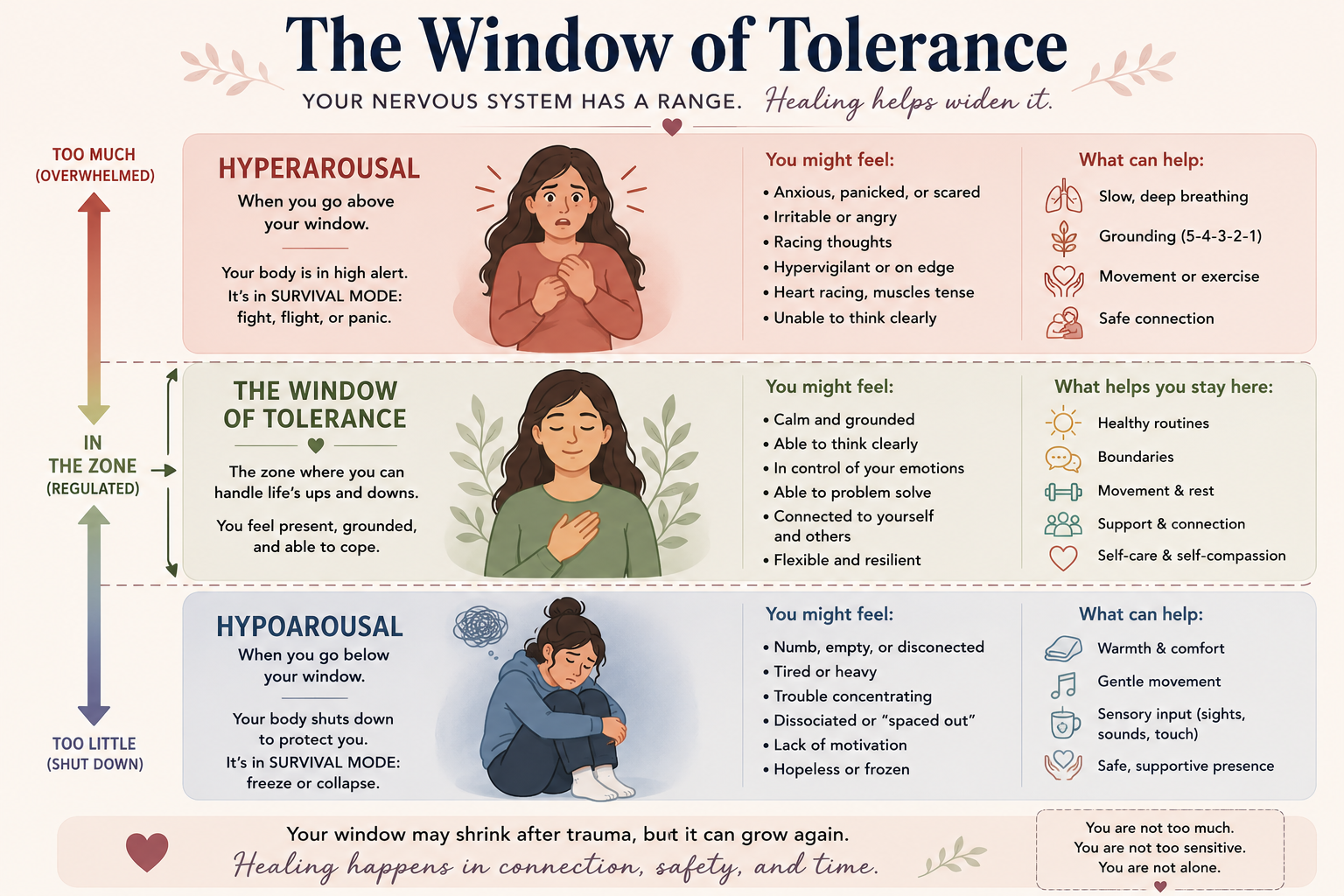
The Nervous System and Trauma
One of the biggest misconceptions about trauma is that it is "all in your head."
It isn't.
Trauma affects your entire nervous system.
This is why survivors often experience symptoms that seem unrelated to the traumatic event itself. Racing heart, chronic muscle tension, stomach problems, panic attacks, difficulty sleeping, emotional numbness, and even changes in sexual functioning are not signs that something is "wrong" with you—they are signs that your nervous system is trying to protect you.
Understanding how the nervous system works can help explain why trauma feels so physical and why healing involves more than simply "thinking differently."
What Is the Nervous System?
The nervous system is your body's communication network.
It constantly gathers information from both your environment and your body, helping you respond to everything from a warm hug to a dangerous situation.
Its primary job is simple:
Keep you alive.
When your nervous system senses safety, your body is free to rest, connect with others, digest food, think clearly, and enjoy life.
When it senses danger, it shifts into survival mode.
This happens automatically and often before you are consciously aware of it.
The Autonomic Nervous System
The part of the nervous system most involved in trauma is called the autonomic nervous system.
It controls many automatic body functions, including:
Heart rate
Breathing
Blood pressure
Digestion
Muscle tension
Sweating
Sexual arousal
Hormone release
You don't consciously tell your heart to beat faster during a frightening situation.
Your nervous system does that for you.
The autonomic nervous system has two primary branches that help keep you alive.
The Sympathetic Nervous System: The Accelerator
The sympathetic nervous system prepares your body to respond to danger.
Think of it as your body's accelerator pedal.
When activated, it releases stress hormones such as adrenaline and cortisol, causing your body to prepare for action.
You may notice:
Faster heart rate.
Rapid breathing.
Increased muscle tension.
Sweaty palms.
Dilated pupils.
Feeling alert or on edge.
Racing thoughts.
Increased energy.
These changes are extremely helpful during genuine danger because they prepare you to fight or flee.
After trauma, however, the sympathetic nervous system may activate even when you are objectively safe.
This is why survivors sometimes experience panic attacks, anxiety, or intense fear without understanding why.
The Parasympathetic Nervous System: The Brake
The parasympathetic nervous system helps your body recover after stress.
Think of it as your body's brake pedal.
When activated, it slows the heart rate, relaxes muscles, supports digestion, and helps you return to a state of calm.
When functioning well, it allows you to:
Feel relaxed.
Digest food comfortably.
Sleep.
Connect with others.
Think clearly.
Experience intimacy.
Recover after stressful events.
For many trauma survivors, this calming system has difficulty fully engaging because the brain continues scanning for danger.
The Vagus Nerve
One of the most important parts of the parasympathetic nervous system is the vagus nerve.
The vagus nerve connects the brain with many organs throughout the body, including the heart, lungs, digestive system, and vocal cords.
It plays an important role in:
Emotional regulation.
Heart rate.
Breathing.
Digestion.
Facial expression.
Voice.
Social connection.
Feelings of safety.
When the vagus nerve is functioning well, it helps us feel calm, connected, and able to engage with the people around us.
When trauma overwhelms the nervous system, these calming pathways may become less effective, making it harder to return to a state of safety.
Why Trauma Feels Physical
Many survivors are surprised by how physical trauma feels.
They may experience:
Chronic muscle tension.
Jaw clenching.
Headaches.
Digestive problems.
Fatigue.
Difficulty sleeping.
Increased startle response.
Chronic pain.
Dizziness.
Rapid heartbeat.
Chest tightness.
Difficulty breathing.
These symptoms are not imagined.
They are the result of a nervous system that continues preparing for danger long after the traumatic event has ended.
Trauma and Sexual Functioning
The nervous system also plays a critical role in sexual health.
Healthy sexual functioning requires the body to feel safe enough to shift out of survival mode.
When the nervous system remains activated, survivors may experience:
Difficulty becoming aroused.
Vaginismus.
Difficulty reaching orgasm.
Emotional disconnection during intimacy.
Fear of physical touch.
This is not because the body is "broken."
It is because the nervous system is prioritizing survival over pleasure.
From a biological perspective, feeling sexually responsive while your brain believes you are in danger would actually be unsafe.
Healing often involves teaching the nervous system that intimacy can once again become associated with safety rather than threat.
The Nervous System Can Learn Safety Again
Perhaps the most hopeful aspect of trauma recovery is that the nervous system is adaptable.
Just as it learned to stay on high alert after trauma, it can also learn to recognize safety again.
This process takes time.
Healing is often gradual and occurs through repeated experiences of safety, predictability, and connection.
Evidence-based therapies such as Eye Movement Desensitization and Reprocessing (EMDR), somatic therapies, mindfulness practices, grounding exercises, breathing techniques, and trauma-informed psychotherapy all work, in different ways, to help regulate the nervous system.
As survivors heal, many notice they are able to:
Calm down more quickly.
Feel safer in relationships.
Experience fewer panic attacks.
Sleep more peacefully.
Feel more connected to their bodies.
Enjoy intimacy again.
Recover from stress more easily.
Feel present instead of constantly on guard.
Healing is not about convincing yourself that you're safe.
It is about helping your nervous system experience safety again.
Your body has spent time learning to survive.
With patience, support, and evidence-based treatment, it can also learn to feel safe.

Why Trauma Responses Are Not a Choice
One of the greatest sources of shame for survivors of sexual trauma is believing they should have reacted differently.
Many people replay the event over and over, asking themselves:
"Why didn't I fight back?"
"Why couldn't I scream?"
"Why did I freeze?"
"Why did I go along with it?"
"Why didn't I leave sooner?"
"Why did I stay in the relationship?"
"Why do I still react this way years later?"
These questions are understandable.
But they are based on one incorrect assumption:
That trauma responses are conscious choices.
They are not.
Trauma responses are automatic biological survival responses controlled by the brain and nervous system. They occur long before your thinking brain has time to decide what to do.
Your body wasn't failing you.
It was trying to protect you.
Your Brain Prioritizes Survival, Not Logic
When the brain detects danger, it immediately shifts into survival mode.
The amygdala—the brain's alarm system—can activate in milliseconds, preparing your body to fight, flee, freeze, or fawn before your prefrontal cortex (the thinking part of your brain) has fully processed what is happening.
This means your nervous system begins making survival decisions before you consciously realize you're in danger.
From an evolutionary perspective, this makes sense.
If our ancestors had paused to carefully analyze every threat before reacting, they might not have survived.
Your brain evolved to react first and think later.
You Can't Simply "Choose" a Different Response
Many survivors believe they should have been able to override their body's reactions.
The reality is that once your nervous system enters survival mode, voluntary control becomes much more limited.
For example:
You cannot simply decide that your heart should stop racing.
You cannot instantly slow your breathing through willpower alone.
You cannot force your muscles to relax while your brain believes you are in danger.
You cannot simply "choose" not to freeze if your nervous system has determined that freezing offers the best chance of survival.
The same brain that controls your heartbeat, breathing, and stress hormones is also coordinating your survival response.
These reactions happen automatically because they are designed to keep you alive.
The Body Remembers What the Mind Tries to Forget
One of the reasons trauma can feel so confusing is that your body often reacts before your conscious mind understands why.
You may know logically that you're safe, yet your body responds as if danger is happening again.
For example, you might notice:
Your heart racing when someone touches your shoulder.
Feeling panicked during intimacy with a loving partner.
Freezing during a medical examination.
Becoming overwhelmed by a familiar smell.
Feeling anxious when someone raises their voice.
These reactions are not choices.
They are learned survival responses stored within your nervous system.
Your brain is attempting to protect you from experiencing harm again.
Why Survivors Blame Themselves
Humans naturally want to believe we have control over difficult experiences.
After trauma, many survivors think:
"If I had fought harder..."
"If I had screamed..."
"If I had left sooner..."
"If I had recognized the warning signs..."
"If I had trusted my instincts..."
These thoughts create the illusion that the outcome could have been completely controlled.
While reflecting on experiences is normal, excessive self-blame often becomes another painful consequence of trauma.
The responsibility for sexual violence always belongs to the person who chose to violate another person's boundaries.
Not the person whose nervous system responded exactly as it was designed to.
Survival Responses Continue After the Trauma Ends
Many survivors assume that once the traumatic event is over, their body should immediately return to normal.
Unfortunately, trauma doesn't always work that way.
After trauma, the brain often continues scanning for danger.
This is why survivors may continue experiencing:
Hypervigilance.
Startle responses.
Panic attacks.
Emotional numbness.
Dissociation.
Difficulty trusting others.
Sleep disturbances.
Anxiety.
Fear during intimacy.
Chronic muscle tension.
These ongoing reactions are not evidence that someone is "stuck" or "broken."
They are signs that the nervous system is still trying to protect them.
Healing Is About Retraining the Nervous System
Because trauma responses are automatic, healing is not about forcing yourself to "get over it."
It is about helping your brain and nervous system learn that the danger has passed.
This is why trauma treatment focuses on creating new experiences of safety rather than simply telling yourself to think differently.
Evidence-based treatments such as Eye Movement Desensitization and Reprocessing (EMDR), somatic therapies, mindfulness practices, grounding exercises, and other trauma-informed approaches help the brain process traumatic memories and reduce the nervous system's need to stay in survival mode.
As healing occurs, many survivors notice that their automatic reactions gradually become less intense.
Their body begins learning something it may not have believed for a long time:
"I am safe now."
Replace Self-Blame With Self-Compassion
Perhaps the most important takeaway from understanding trauma is this:
Your survival responses were never evidence of weakness.
They were evidence that your brain and nervous system were doing everything they could to keep you alive.
You did not choose to freeze.
You did not choose to panic.
You did not choose to dissociate.
You did not choose to have nightmares.
You did not choose to struggle with intimacy afterward.
These were adaptations—your body's best attempt to survive an overwhelming experience.
Healing often begins when survivors stop asking,
"What's wrong with me?"
and begin asking,
"What happened to me, and how can I help my nervous system heal?"
That shift—from self-blame to self-compassion—can become one of the most important turning points in recovery.
Part 3: How Sexual Trauma Can Affect Your Life
Emotional Effects of Sexual Trauma
Sexual trauma affects much more than the event itself.
For many survivors, the emotional effects continue long after the trauma has ended. Some people notice changes immediately, while others don't experience significant emotional symptoms until months or even years later. There is no "correct" timeline for trauma. Every survivor's healing journey is unique.
One of the most important things to understand is that these emotional responses are not signs of weakness or personal failure. They are normal reactions to abnormal experiences. Your brain and nervous system are doing what they were designed to do—protect you after something overwhelming has happened.
Some survivors experience only a few emotional symptoms, while others experience many. Symptoms may come and go over time and often change as life circumstances change.
Anxiety
Anxiety is one of the most common emotional responses after sexual trauma.
Because trauma teaches the brain that the world may not be safe, survivors often remain alert for signs of danger long after the trauma has ended.
You may experience:
Constant worry
Feeling "on edge"
Racing thoughts
Muscle tension
Difficulty relaxing
Difficulty concentrating
Trouble sleeping
Feeling easily startled
Even when you know you are safe, your nervous system may continue responding as though danger is still present.
Fear
Many survivors develop fears that were not present before the trauma.
These fears may include:
Fear of being alone
Fear of strangers
Fear of dating
Fear of intimacy
Fear of conflict
Fear of certain places
Fear of physical touch
Fear of losing control
Fear that the trauma will happen again
These fears are your brain's attempt to prevent future harm.
Shame
Shame is one of the most painful emotions survivors experience.
Unlike guilt, which says, "I did something wrong," shame says:
"Something is wrong with me."
Many survivors blame themselves for:
Freezing
Not fighting back
Staying in the relationship
Trusting the person
Drinking alcohol
Missing warning signs
Their body's physical responses during the assault
These beliefs often develop despite the fact that responsibility belongs entirely to the person who caused the harm.
Healing often involves replacing shame with self-compassion.
Guilt
Many survivors feel guilty about things they could not control.
They may believe they should have:
Said no more forcefully
Screamed
Left sooner
Reported the assault
Protected someone else
Seen the warning signs
These thoughts are understandable, but they often reflect hindsight rather than the reality of how trauma affects the brain and nervous system.
Anger
Anger is a healthy and common response to having your boundaries violated.
Some survivors feel angry immediately.
Others do not experience anger until years later, after they begin recognizing the full impact of what happened.
Anger may be directed toward:
The person responsible
Friends or family who did not protect them
Institutions that failed them
Society
Themselves
Their own bodies
Learning to safely experience and express anger is often an important part of recovery.
Sadness and Grief
Sexual trauma often involves grieving more than the event itself.
Many survivors grieve:
Their sense of safety
Their trust in others
Their innocence
Their previous identity
Lost relationships
Missed opportunities
The life they imagined before the trauma
Grief is a natural response to loss, and healing often includes allowing space for these emotions.
Depression
Some survivors develop symptoms of depression after trauma.
These may include:
Persistent sadness
Loss of interest in activities
Feeling emotionally numb
Hopelessness
Low energy
Difficulty concentrating
Changes in appetite
Changes in sleep
Feeling disconnected from life
Depression can develop immediately after trauma or emerge much later.
Emotional Numbness
Not everyone cries after trauma.
Some survivors feel almost nothing.
Emotional numbness is another protective response of the nervous system.
You may notice:
Feeling emotionally flat
Difficulty crying
Feeling disconnected from your emotions
Feeling detached from loved ones
Difficulty experiencing joy
Feeling like you're "going through the motions"
This does not mean you are uncaring.
It often means your nervous system has temporarily reduced emotional awareness in order to protect you.
Self-Blame
Many survivors become their own harshest critics.
Self-blame often sounds like:
"It was my fault."
"I should have known better."
"I let it happen."
"I shouldn't have trusted them."
"I should be over this by now."
Self-blame creates the illusion of control. If we convince ourselves the trauma happened because of something we did, it can feel safer to believe we can prevent it from happening again.
The reality is much simpler:
The responsibility belongs to the person who chose to violate your boundaries.
Loss of Trust
After sexual trauma, trusting others may feel difficult.
Survivors may struggle to trust:
Romantic partners
Friends
Family members
Authority figures
Medical professionals
Therapists
Even themselves
Rebuilding trust is often a gradual process that develops through repeated experiences of safety and consistency.
Emotional Triggers
Many survivors notice that certain situations suddenly bring back intense emotions.
Common emotional triggers include:
Certain smells
Music
Particular dates
Medical appointments
Sexual intimacy
Raised voices
Alcohol
Specific locations
News stories
Movies or television shows
These emotional reactions are not signs that you are "moving backward."
They are reminders that your brain is still learning the difference between past danger and present safety.

Physical Effects of Sexual Trauma
Sexual trauma affects far more than your emotions.
Because trauma changes how the brain and nervous system respond to stress, many survivors experience physical symptoms that continue long after the traumatic event has ended. These symptoms are real, common, and rooted in biology—not signs that you are "imagining things" or that the trauma is "all in your head."
When your brain perceives danger, it activates your body's survival response. Heart rate increases, muscles tense, stress hormones are released, and your nervous system prepares to protect you. For some survivors, this state of heightened alert continues long after the danger has passed, contributing to ongoing physical symptoms.
The body often remembers what the mind is trying to forget.
Chronic Muscle Tension
One of the most common physical effects of trauma is persistent muscle tension.
Many survivors unconsciously hold tension throughout the day, particularly in the:
Neck
Shoulders
Jaw
Back
Pelvic floor
Hips
Over time, this chronic tension can contribute to pain, headaches, fatigue, and restricted movement.
Some people don't realize how tense their body has become until they begin learning relaxation or grounding techniques in therapy.
Chronic Pain
Research has found that survivors of sexual trauma are more likely to experience chronic pain conditions.
These may include:
Pelvic pain
Lower back pain
Neck pain
Headaches
Migraines
Fibromyalgia
Widespread muscle pain
Temporomandibular joint (TMJ) pain
Pain after trauma does not necessarily mean there is ongoing injury.
Sometimes the nervous system becomes highly sensitive, causing the brain to interpret normal sensations as painful. This is sometimes referred to as central sensitization, where the nervous system becomes overprotective and amplifies pain signals.
Sleep Problems
Feeling safe is essential for restful sleep.
When the nervous system remains on high alert, many survivors experience:
Difficulty falling asleep
Waking frequently during the night
Nightmares
Night terrors
Restless sleep
Feeling exhausted despite sleeping
Fear of sleeping alone
Difficulty returning to sleep after waking
Poor sleep can also make anxiety, depression, chronic pain, and emotional regulation more difficult.
Fatigue
Living in survival mode is exhausting.
Many survivors describe feeling physically drained, even when they have not been particularly active.
Chronic activation of the stress response can contribute to:
Low energy
Mental exhaustion
Feeling physically heavy
Difficulty getting out of bed
Feeling burned out
Reduced motivation
Fatigue is not laziness.
It is often a sign that your nervous system has been working overtime to protect you.
Digestive Problems
The brain and digestive system communicate constantly through the gut-brain connection.
When the nervous system is stuck in survival mode, digestion often slows or becomes disrupted.
Survivors may experience:
Stomach aches
Nausea
Irritable bowel syndrome (IBS)
Constipation
Diarrhea
Acid reflux
Appetite changes
Bloating
Stress hormones can affect digestion, which is why many people notice stomach symptoms during periods of anxiety or after trauma reminders.
Headaches and Migraines
Trauma-related muscle tension, chronic stress, and nervous system activation can contribute to frequent headaches or migraines.
Some survivors notice headaches:
After nightmares
Following stressful conversations
Around trauma anniversaries
After medical appointments
During periods of emotional overwhelm
Learning nervous system regulation skills often helps reduce the frequency or intensity of these symptoms.
Increased Startle Response
Many survivors notice they startle more easily after trauma.
You may find yourself reacting strongly to:
Loud noises
Someone entering the room unexpectedly
A door slamming
Someone touching you unexpectedly
Hearing footsteps behind you
This happens because the brain's alarm system—the amygdala—has become more sensitive to potential danger.
Rapid Heart Rate and Panic Symptoms
The body's stress response can produce powerful physical sensations, including:
Racing heart
Chest tightness
Sweating
Shaking
Shortness of breath
Dizziness
Feeling faint
Tingling sensations
These symptoms can be frightening and sometimes lead people to believe they are having a medical emergency.
Although panic symptoms are real and deserve medical evaluation when appropriate, they are often the result of a nervous system responding to perceived danger rather than actual physical illness.
Pelvic Floor Dysfunction
The pelvic floor muscles often respond to trauma by becoming tense and protective.
For some survivors, this chronic guarding can contribute to:
Pelvic pain
Difficulty using tampons
Pain during gynecological examinations
Difficulty emptying the bladder
Constipation
Pain with bowel movements
Pelvic floor physical therapy, combined with trauma-informed care, can be an important part of recovery for many survivors.
Changes in Sexual Functioning
Because healthy sexual functioning depends on feeling safe, trauma can affect many aspects of sexual health.
Survivors may experience:
Difficulty becoming aroused
Pain during sex
Vaginismus
Vulvodynia
Erectile dysfunction
Difficulty reaching orgasm
Delayed ejaculation
Premature ejaculation related to anxiety
Feeling emotionally disconnected during intimacy
These changes are common and often improve as the nervous system heals.
Immune System Changes
Chronic stress can also affect the immune system.
Some survivors notice:
Getting sick more often
Taking longer to recover from illness
Increased inflammation
Flare-ups of autoimmune conditions
Slower wound healing
While trauma is not the sole cause of these conditions, chronic activation of the body's stress response can contribute to overall physical health.
Why These Symptoms Happen
Many survivors worry that their symptoms mean something is "wrong" with them.
The reality is that these physical reactions often reflect a nervous system that is doing exactly what it was designed to do—protect you.
After trauma, the brain becomes more sensitive to possible danger. As a result, the body may continue preparing for threats even when the danger has passed.
This prolonged state of survival can affect nearly every system in the body, including the muscles, digestive system, cardiovascular system, immune system, and reproductive system.
Understanding this can help replace fear and self-blame with compassion.
Your body is not working against you.
It is trying to keep you safe.

Relationship Effects of Sexual Trauma
Sexual trauma can affect every part of a person's life—including their relationships.
For many survivors, one of the most painful losses after trauma is the feeling that relationships no longer feel as safe, easy, or fulfilling as they once did. Trust may become difficult. Vulnerability can feel frightening. Physical affection may trigger anxiety, and even healthy, loving relationships can feel overwhelming at times.
These changes are not signs that you are incapable of having healthy relationships.
They are common responses from a brain and nervous system that have learned to associate closeness with danger.
The good news is that relationships can heal. With time, self-compassion, and trauma-informed support, many survivors are able to rebuild trust, intimacy, and meaningful connection.
Difficulty Trusting Others
Trust is often one of the first things trauma takes away.
When someone violates your body, boundaries, or sense of safety, your brain naturally becomes more cautious about letting people get close again.
You may find yourself:
Assuming people have hidden motives.
Expecting to be hurt or betrayed.
Feeling suspicious even in healthy relationships.
Keeping emotional distance.
Struggling to believe compliments or reassurance.
Constantly looking for signs that someone might leave or hurt you.
These reactions are your brain's attempt to prevent future pain.
Difficulty Trusting Yourself
Many survivors also lose trust in themselves.
You may wonder:
"How did I not see the warning signs?"
"Can I trust my judgment?"
"What if I make the same mistake again?"
"Why didn't I leave sooner?"
Trauma often causes survivors to question their instincts, memories, and decision-making.
Learning to trust yourself again is an important part of healing.
Fear of Vulnerability
Healthy relationships require vulnerability.
Trauma teaches the opposite.
Many survivors begin protecting themselves by avoiding emotional closeness because closeness once led to pain.
You may notice yourself:
Keeping conversations superficial.
Avoiding emotional intimacy.
Struggling to ask for help.
Hiding your feelings.
Feeling uncomfortable when someone cares deeply about you.
Pulling away when relationships become serious.
These protective behaviors often develop without conscious awareness.
Difficulty Communicating Needs
Many survivors learn that expressing needs was unsafe.
As a result, they may struggle to:
Say no.
Set boundaries.
Ask for reassurance.
Express sexual preferences.
Tell a partner when something feels uncomfortable.
Speak up during conflict.
Instead, survivors may stay silent, avoid conflict, or prioritize everyone else's needs above their own.
These patterns are often rooted in survival—not personality.
Fear of Conflict
For some survivors, disagreements feel far more threatening than they actually are.
Even healthy conflict may trigger:
Panic.
Shutting down.
Crying.
Freezing.
Avoiding difficult conversations.
Agreeing just to end the discussion.
Leaving emotionally before the conversation begins.
Your nervous system may react to conflict as though it is dangerous, even when your partner is communicating respectfully.
People-Pleasing and the Fawn Response
Many survivors become chronic people-pleasers.
They may:
Put others' needs before their own.
Have difficulty saying no.
Feel responsible for other people's emotions.
Apologize excessively.
Avoid disappointing others.
Stay in unhealthy relationships.
Ignore their own boundaries.
These behaviors often develop from the fawn response, where the nervous system learns that keeping others happy increases safety.
Although people-pleasing may have once been protective, it can become exhausting over time.
Difficulty With Physical Affection
Not all survivors struggle with sexual intimacy alone.
Some also find non-sexual touch challenging.
This may include:
Hugging.
Holding hands.
Cuddling.
Sitting close together.
Unexpected touch.
Kissing.
For some people, even affectionate touch can activate the nervous system because the body has learned to associate closeness with danger.
Isolation
Trauma often causes survivors to withdraw from others.
You may notice yourself:
Spending more time alone.
Avoiding dating.
Canceling plans.
Feeling disconnected from friends.
Feeling misunderstood.
Believing no one could understand your experience.
Isolation can feel protective in the short term but often increases loneliness over time.
Difficulty Feeling Emotionally Safe
Many survivors describe always feeling "on guard."
Even in healthy relationships, they may struggle to fully relax.
You may find yourself:
Watching for signs of rejection.
Expecting betrayal.
Preparing for the relationship to end.
Feeling uncomfortable when things are going well.
Overanalyzing text messages or conversations.
Needing constant reassurance.
These reactions reflect a nervous system that is trying to anticipate danger before it happens.
Changes in Attachment
Trauma can influence the way people connect with others.
Some survivors become more anxious in relationships and may:
Fear abandonment.
Seek constant reassurance.
Worry about being rejected.
Others become more avoidant and may:
Keep emotional distance.
Value independence above connection.
Avoid relying on others.
End relationships before becoming vulnerable.
Some people experience both patterns at different times.
These attachment changes are understandable adaptations to trauma—not permanent personality traits.
Parenting After Sexual Trauma
Survivors who become parents often notice that trauma affects parenting in unexpected ways.
Some become highly protective.
Others worry about repeating harmful patterns or struggle when their child's developmental stages remind them of their own trauma.
Many survivors also find that pregnancy, childbirth, breastfeeding, diaper changes, or discussions about body safety can activate unresolved trauma.
These experiences are common and can be addressed through trauma-informed therapy.
Healthy Relationships Can Feel Uncomfortable at First
One of the more surprising parts of healing is that healthy relationships may initially feel unfamiliar.
If your nervous system learned that love included fear, manipulation, or unpredictability, consistency may feel strange.
A respectful partner may seem "boring."
Healthy boundaries may feel unfamiliar.
Kindness may even feel suspicious.
This doesn't mean healthy relationships are wrong.
It means your nervous system is learning a new definition of safety.
Healing Relationships After Trauma
Healing is not about becoming the person you were before the trauma.
It is about creating relationships that are built on safety, trust, honesty, respect, and mutual consent.
Many survivors find healing through:
Individual trauma therapy.
EMDR.
Learning healthy communication skills.
Practicing boundaries.
Developing self-compassion.
Gradually rebuilding trust.
Creating positive experiences of emotional and physical safety.
Healing relationships takes time.
There may be setbacks along the way, but each experience of safety teaches your brain that connection does not always lead to harm.
Healthy relationships do not require perfection.
They require safety, respect, honesty, communication, and repair.
And those are all things that can be learned.

Sexual Effects of Sexual Trauma
One of the most misunderstood effects of sexual trauma is how it can affect a person's sexuality.
Many survivors worry that something is "wrong" with them because sex no longer feels the way it once did—or perhaps never has. Some lose interest in sex altogether, while others feel disconnected during intimacy. Some experience pain, difficulty becoming aroused, or trouble reaching orgasm. Others notice changes in their erections, ejaculation, or sexual desire.
These reactions are incredibly common.
Sexual functioning depends on your brain and nervous system feeling safe. When the brain believes you are in danger, it shifts its focus toward survival—not pleasure.
The good news is that these changes are often treatable. As your brain and nervous system heal, your relationship with intimacy and sexuality can heal as well.
Low Sexual Desire
Many survivors notice a significant decrease in sexual desire after trauma.
You may experience:
Avoiding sexual situations.
Feeling indifferent toward intimacy.
Feeling disconnected from your sexuality.
Wanting emotional closeness but not sexual touch.
This is one of the nervous system's ways of protecting you.
If your brain has learned to associate sex with danger, reducing sexual desire can become an adaptive survival strategy.
Low desire after trauma is not a sign that you are broken or incapable of having a healthy sex life.
Difficulty Becoming Aroused
Even when survivors want to be intimate, their bodies may not respond the way they expect.
You may experience:
Difficulty becoming physically aroused.
Feeling emotionally present but physically unresponsive.
Feeling physically aroused but emotionally disconnected.
Needing significantly more time to become aroused.
Losing arousal during intimacy.
Arousal depends on the parasympathetic nervous system—the part of the nervous system responsible for rest, relaxation, and connection.
If your brain is scanning for danger, it is much more difficult for your body to shift into a state that supports sexual arousal.
Pain During Sex
Painful sex is a common but often overlooked consequence of sexual trauma.
Survivors may experience:
Burning.
Stinging.
Tightness.
Pelvic pain.
Pain with penetration.
Pain during or after intercourse.
Pain during gynecological exams.
Difficulty inserting tampons.
For some people, the pelvic floor muscles become chronically tense after trauma, creating involuntary muscle guarding.
Pain is not "all in your head."
It is a real physical experience that often reflects changes in the nervous system, pelvic floor muscles, and brain's perception of safety.
Difficulty Reaching Orgasm
Some survivors find that orgasm becomes difficult—or impossible.
You may notice:
Feeling close to orgasm but never reaching it.
Losing arousal just before orgasm.
Becoming distracted by anxious thoughts.
Feeling emotionally disconnected during pleasure.
Feeling guilty or ashamed when experiencing pleasure.
Orgasm requires the ability to relax, stay present, and allow the body to feel safe.
When the brain remains focused on survival, orgasm can become much more difficult.
Erectile Dysfunction
Sexual trauma can affect people with penises as well.
Some survivors experience:
Difficulty maintaining an erection.
Losing erections during intimacy.
Increased performance anxiety.
Fear of sexual situations.
This is not a sign of weakness or a lack of attraction.
Stress, anxiety, hypervigilance, and trauma can interfere with the complex interaction between the brain, nervous system, blood flow, hormones, and emotions that make erections possible.
Premature or Delayed Ejaculation
Trauma can also affect ejaculation.
Some survivors notice:
Ejaculating sooner than they would like.
Difficulty ejaculating.
Feeling unable to climax with a partner.
Ejaculating only during masturbation.
Feeling anxious about sexual performance.
These changes are often related to nervous system activation rather than physical dysfunction alone.
Dissociation During Sex
Many survivors describe feeling emotionally absent during intimacy.
This is known as dissociation.
You may experience:
Feeling disconnected from your body.
Feeling like you are watching yourself from outside your body.
"Checking out" mentally.
Difficulty remembering parts of sexual experiences.
Feeling numb during intimacy.
Dissociation is an automatic survival response.
It developed to help you survive overwhelming experiences.
Although it may no longer be helpful, it is not something you consciously choose.
Flashbacks During Intimacy
Physical touch, certain positions, smells, sounds, or sensations can sometimes trigger traumatic memories.
Some survivors experience:
Intrusive memories.
Sudden panic.
Feeling like the assault is happening again.
Crying unexpectedly.
Freezing.
Feeling overwhelmed by physical touch.
These reactions can occur even with a loving, safe partner.
They do not mean you are unsafe now.
They mean your nervous system is reacting to reminders of past danger.
Feeling Guilty About Pleasure
One of the most painful experiences for many survivors is feeling guilty when they experience sexual pleasure.
Some wonder:
"Am I allowed to enjoy sex?"
"Does wanting sex mean I'm minimizing what happened?"
"Why do I feel ashamed after consensual intimacy?"
Others may experience involuntary physical arousal during an assault and later believe that this means they somehow consented.
This is not true.
The body can respond automatically to physical stimulation, even during fear or assault.
Physical arousal is a biological reflex.
It is not consent.
It is not enjoyment.
It is not your fault.
Avoidance of Intimacy
For some survivors, avoiding sex feels like the safest option.
You may:
Avoid dating.
Avoid affectionate touch.
End relationships before intimacy develops.
Find excuses to avoid sex.
Feel anxious whenever intimacy is expected.
Avoidance is one way the brain attempts to prevent further emotional pain.
While it may reduce anxiety in the short term, it can also increase loneliness and make healing more difficult over time.
Hypersexuality After Trauma
Not every survivor avoids sex.
Some notice an increase in sexual behavior after trauma.
This may include:
Seeking frequent sexual encounters.
Using sex to feel wanted or validated.
Difficulty saying no to unwanted sexual experiences.
Engaging in sexual activity despite not truly wanting it.
Using sex to cope with emotional pain.
Feeling emotionally disconnected during sexual activity.
For some survivors, sex becomes a way to regain a sense of control, numb difficult emotions, or reconnect with their bodies.
Hypersexuality is not an inevitable consequence of trauma, nor does it occur in every survivor. When it does occur, it should be understood with curiosity and compassion rather than judgment.
write this section: Mental Health After sexual Trauma
Mental Health After Sexual Trauma
Sexual trauma can have a profound impact on mental health.
While every survivor's experience is unique, many people notice emotional, psychological, and behavioral changes after trauma. Some symptoms develop immediately, while others may not appear until months or even years later.
Experiencing mental health challenges after sexual trauma does not mean you are weak, broken, or "going crazy." These reactions are common responses to overwhelming experiences.
The good news is that recovery is possible. With compassionate support and evidence-based treatment, many survivors experience significant healing and go on to build fulfilling, meaningful lives.
Post-Traumatic Stress Disorder (PTSD)
One of the most well-known mental health conditions associated with sexual trauma is Post-Traumatic Stress Disorder (PTSD).
PTSD develops when the brain and nervous system continue responding as though the traumatic event is still happening, even after the danger has passed.
Common symptoms include:
Flashbacks.
Nightmares.
Intrusive memories.
Hypervigilance.
Avoiding reminders of the trauma.
Feeling emotionally numb.
Difficulty sleeping.
Increased startle response.
Irritability.
Difficulty concentrating.
Not everyone who experiences sexual trauma develops PTSD, but it is one of the most common mental health outcomes.
Complex PTSD (C-PTSD)
Some survivors experience repeated or long-term trauma, such as childhood sexual abuse, ongoing abuse within a relationship, trafficking, or repeated sexual exploitation.
These experiences may contribute to Complex Post-Traumatic Stress Disorder (C-PTSD).
In addition to symptoms of PTSD, people with C-PTSD may experience:
Difficulty regulating emotions.
Persistent shame.
Negative beliefs about themselves.
Feeling permanently damaged.
Difficulty trusting others.
Relationship challenges.
Chronic feelings of emptiness.
Dissociation.
Problems with identity or self-worth.
Because the trauma occurred repeatedly over time, healing often involves rebuilding a sense of safety, identity, and connection.
Anxiety Disorders
Anxiety is one of the most common mental health effects of sexual trauma.
Your brain has learned that the world may not always be safe, making it more likely to stay alert for possible danger.
You may experience:
Constant worry.
Feeling on edge.
Racing thoughts.
Muscle tension.
Panic attacks.
Difficulty relaxing.
Fear of being alone.
Fear of intimacy.
Difficulty concentrating.
These reactions reflect a nervous system working overtime to protect you.
Depression
Many survivors experience depression after sexual trauma.
Depression may develop because of grief, loss, shame, isolation, chronic stress, or changes in brain chemistry associated with trauma.
Common symptoms include:
Persistent sadness.
Feeling emotionally numb.
Loss of interest in activities.
Fatigue.
Difficulty concentrating.
Changes in sleep.
Changes in appetite.
Feelings of hopelessness.
Low motivation.
Depression is treatable, and many survivors experience significant improvement with appropriate support.
Panic Disorder
Some survivors begin experiencing panic attacks after trauma.
Panic attacks may include:
Racing heart.
Chest tightness.
Shortness of breath.
Dizziness.
Sweating.
Trembling.
Feeling detached from reality.
Fear of dying or losing control.
Although panic attacks can feel terrifying, they are not dangerous.
They are the result of a nervous system that has become highly sensitive to perceived threats.
Dissociation
Dissociation is a protective response that allows the brain to distance itself from overwhelming experiences.
Survivors may experience:
Feeling detached from their body.
Feeling emotionally numb.
Memory gaps.
Feeling like they are watching themselves from outside their body.
Feeling disconnected from reality.
Losing track of time.
Although dissociation can feel frightening, it developed as a survival strategy during overwhelming experiences.
Obsessive-Compulsive Symptoms
Some survivors notice increased obsessive thoughts or compulsive behaviors after trauma.
They may:
Repeatedly check locks or doors.
Seek excessive reassurance.
Mentally replay traumatic events.
Feel responsible for preventing future harm.
Experience intrusive thoughts about safety or contamination.
For some people, trauma can worsen existing obsessive-compulsive symptoms or contribute to new ones.
Substance Use
Some survivors turn to alcohol or drugs in an attempt to cope with emotional pain.
Substances may temporarily reduce anxiety or numb distressing emotions, but they often make trauma symptoms worse over time.
Recovery involves learning healthier ways to regulate emotions while addressing the underlying trauma.
There is no shame in seeking support for both trauma and substance use at the same time.
Self-Harm
Some survivors engage in self-harm as a way to cope with overwhelming emotional pain, numbness, shame, or feelings that seem impossible to express.
Self-harm is not attention-seeking.
For many people, it represents an attempt to manage distress using the coping strategies available to them at the time.
Healing involves learning safer ways to regulate emotions while addressing the underlying trauma.
Suicidal Thoughts
Some survivors experience thoughts that life is no longer worth living.
These thoughts often arise from overwhelming pain—not because someone truly wants to die, but because they desperately want the suffering to end.
If you have experienced suicidal thoughts, it does not mean you are weak or beyond help.
Recovery is possible, and many people who once believed healing was impossible later describe lives filled with hope, connection, and meaning.
If you are experiencing thoughts of harming yourself or feel unable to keep yourself safe, seek immediate support from a trusted person, a mental health professional, or your local emergency services. You do not have to face this alone.
Eating Disorders and Body Image
Sexual trauma can also affect a person's relationship with food and their body.
Some survivors develop:
Restrictive eating.
Binge eating.
Emotional eating.
Purging behaviors.
Intense body dissatisfaction.
Feeling disconnected from their body.
For some people, changing their body becomes an unconscious attempt to feel safer or regain a sense of control.
Mental Health Conditions Are Treatable
Experiencing mental health symptoms after sexual trauma does not mean they will last forever.
The brain is capable of healing.

Part 4: Why Sex Can Feel Different After Trauma
Changes in Sexual Desire
One of the most common—and often confusing—effects of sexual trauma is a change in sexual desire.
Some survivors notice that their interest in sex decreases significantly after trauma. Others find that their desire increases. Some experience both at different times in their healing journey.
There is no "normal" way to respond.
Your brain and nervous system are trying to adapt to what happened, and those adaptations can affect sexuality in many different ways.
Understanding these changes can help reduce shame and remind survivors that they are not alone.
Low Sexual Desire
For many survivors, sexual desire decreases after trauma.
You may notice that you:
Rarely think about sex.
Avoid sexual situations.
Feel indifferent toward intimacy.
Lose interest in masturbation.
Feel emotionally disconnected from your sexuality.
Want emotional closeness but not sexual touch.
This is a very common trauma response.
When the brain has learned to associate sexual experiences with danger, reducing sexual desire can become one way the nervous system tries to protect you.
It is difficult to feel desire when your brain believes you need to focus on survival.
Low desire after trauma is not a sign that you are broken, that you no longer love your partner, or that you will never enjoy sex again.
Increased Sexual Desire
Not everyone experiences lower desire.
Some survivors notice that they think about sex more often or seek out sexual experiences more frequently after trauma.
This can be confusing and sometimes deeply shame-inducing.
However, increased sexual desire does not mean someone wanted the trauma or was unaffected by it.
For some survivors, sexual behavior becomes a way to:
Feel in control.
Regain ownership of their body.
Seek comfort or connection.
Feel wanted or valued.
Distract themselves from painful emotions.
Temporarily numb anxiety or distress.
Others may feel compelled to engage in sexual activity even when they do not truly want to because their nervous system has learned that compliance increases safety.
Increased sexual behavior after trauma is not uncommon, and it deserves compassion—not judgment.
Fluctuating Desire
Many survivors experience desire that changes over time.
For example, someone may:
Avoid sex for months or years.
Suddenly experience an increase in desire.
Feel interested in sex one day and completely shut down the next.
Want sex emotionally but find their body unresponsive.
Feel physically aroused while emotionally disconnected.
These fluctuations can feel confusing, but they are often a reflection of the nervous system moving in and out of different states of regulation.
Healing is rarely a straight line.
Why Trauma Changes Desire
Healthy sexual desire depends on feeling safe.
The brain constantly asks one important question:
"Am I safe?"
If the answer is no—or even "I'm not sure"—the brain shifts resources toward protection rather than pleasure.
Trauma can lead to:
An overactive fear response.
Hypervigilance.
Difficulty relaxing.
Emotional disconnection.
Pelvic floor muscle tension.
Increased stress hormones.
Fear of vulnerability.
All of these factors can affect sexual desire.
Your body is not working against you.
It is trying to keep you safe.
Changes in Desire Do Not Measure Love
One of the biggest misconceptions about sexual desire is that it reflects how much someone loves or is attracted to their partner.
It does not.
A survivor may deeply love their partner while still experiencing:
Low libido.
Fear during intimacy.
Difficulty becoming aroused.
Emotional shutdown during sex.
Avoidance of sexual activity.
Likewise, someone with increased sexual desire after trauma is not "less traumatized."
Trauma affects everyone differently.
Your level of desire is not a measure of your love, your healing, or the severity of your trauma.
Desire Can Return
Many survivors worry that they have permanently lost their sexuality.
Fortunately, research and clinical experience suggest otherwise.
As trauma heals and the nervous system begins to feel safe again, many people notice gradual improvements in:
Sexual desire.
Arousal.
Comfort with intimacy.
Pleasure.
Emotional connection during sex.
Confidence in their bodies.
Healing does not always mean returning to the exact sexuality you had before the trauma.
Instead, many survivors discover a new relationship with sexuality—one based on safety, consent, curiosity, pleasure, and choice.
Supporting Yourself Through Changes in Desire
If your sexual desire has changed after trauma, consider approaching yourself with curiosity instead of criticism.
Ask yourself:
What helps me feel emotionally safe?
When do I feel most connected to my body?
What situations increase or decrease my sense of safety?
Am I responding from fear, obligation, or genuine desire?
What would help intimacy feel more comfortable?
There is no deadline for healing.
Your sexuality belongs to you, and you have the right to rediscover it at your own pace.
Working with a trauma-informed therapist, sex therapist, or pelvic floor physical therapist can also help you better understand these changes and develop a path toward healing.

Pain During Sex
Pain during sex is one of the most common—but least talked about—effects of sexual trauma.
Many survivors feel embarrassed, confused, or frustrated when intimacy becomes painful. Some wonder if the pain is "just in their head," while others worry that their bodies are permanently damaged.
The truth is that pain during sex is a real and common response to trauma.
Sexual trauma can affect the brain, nervous system, pelvic floor muscles, hormones, and emotions. All of these systems work together during sexual activity. When one or more of them is disrupted by trauma, pain can occur.
The encouraging news is that pain during sex is often treatable. With the right care, many survivors experience significant improvement and are able to enjoy comfortable, pleasurable intimacy again.
How Trauma Can Cause Pain During Sex
Healthy sexual functioning depends on the body feeling safe.
When the brain senses safety, the nervous system allows the pelvic floor muscles to relax, blood flow increases to the genitals, natural lubrication improves, and the body becomes more receptive to sexual touch.
After sexual trauma, the brain may continue interpreting intimacy as a potential threat.
As a result, the body may automatically respond by:
Tightening the pelvic floor muscles.
Reducing natural lubrication.
Increasing muscle guarding.
Becoming hypervigilant.
Releasing stress hormones.
Triggering fear or panic during intimacy.
These are protective survival responses—not conscious choices.
Your body is trying to keep you safe.
Common Types of Sexual Pain
Pain during sex can feel different for different people.
Some survivors describe:
Burning.
Stinging.
Sharp pain.
Deep pelvic pain.
Aching.
Tightness.
Pressure.
Muscle spasms.
Pain only during penetration.
Pain that continues after sex.
The location, intensity, and timing of pain can vary from person to person.
Vaginismus
One condition that commonly develops after sexual trauma is vaginismus.
Vaginismus occurs when the pelvic floor muscles involuntarily tighten around the vaginal opening, making penetration difficult, painful, or impossible.
Because the tightening happens automatically, survivors cannot simply "relax" their muscles through willpower alone.
Vaginismus may affect:
Sexual intercourse.
Tampon insertion.
Gynecological examinations.
Pelvic floor therapy.
Use of vaginal dilators.
Although trauma is one possible cause, vaginismus can also occur for other medical or psychological reasons.
The important thing to remember is that it is a treatable condition.
Vulvodynia
Some survivors experience vulvodynia, which is chronic pain affecting the vulva without an identifiable infection or injury.
Symptoms may include:
Burning.
Stinging.
Rawness.
Tenderness.
Irritation.
Pain during sitting, exercise, or sexual activity.
Researchers believe that changes in the nervous system, inflammation, pelvic floor dysfunction, and past trauma may all contribute to vulvodynia in some individuals.
Pelvic Floor Dysfunction
The pelvic floor is a group of muscles that supports the bladder, bowel, and reproductive organs.
Following trauma, these muscles often remain chronically tense.
This tension may contribute to:
Difficulty inserting tampons.
Pain during pelvic exams.
Bladder symptoms.
Constipation.
Lower back pain.
Hip pain.
Pelvic pressure.
Many survivors are surprised to learn that their pelvic floor muscles have been "guarding" for months or even years.
Pain Can Affect Anyone
Although pain during penetration is often discussed in relation to women, survivors of all genders can experience pain during sexual activity.
People of any gender may experience:
Genital pain.
Pelvic floor tension.
Muscle guarding.
Pain during certain sexual activities.
Anxiety-related physical discomfort.
Difficulty relaxing during intimacy.
Sexual trauma affects the nervous system—not just one part of the body.
Fear and Pain Can Create a Cycle
Pain and fear often reinforce one another.
For example:
A painful sexual experience may increase anxiety before the next sexual encounter.
That anxiety causes the body to tense.
The increased muscle tension makes pain more likely.
The painful experience then reinforces the brain's belief that intimacy is unsafe.
Over time, this cycle can become stronger if left untreated.
The good news is that this cycle can also be interrupted.
As the brain learns that intimacy can be safe, pain often decreases.
Pain Is Never "Just in Your Head"
One of the most harmful myths about painful sex is that it is "psychological."
While the brain and nervous system certainly influence pain, that does not mean the pain is imagined.
Pain is always a real experience.
Trauma changes how the brain processes pain signals, how muscles respond, and how the nervous system interprets touch.
Understanding this helps many survivors replace shame with self-compassion.
Treatment for Pain During Sex
Recovery often involves addressing both the body and the nervous system.
Treatment may include:
Pelvic floor physical therapy.
Trauma-informed psychotherapy.
Eye Movement Desensitization and Reprocessing (EMDR).
Vaginal dilator therapy (when appropriate).
Mindfulness and relaxation exercises.
Breathing techniques.
Education about the nervous system.
Medical evaluation to rule out other causes of pain.
Lubricants or other treatments recommended by a healthcare provider.
Because pain during sex can have multiple contributing factors, many survivors benefit from working with a team that may include a physician, pelvic floor physical therapist, and trauma-informed sex therapist.

Difficulty Becoming Aroused
After sexual trauma, many survivors notice that becoming sexually aroused feels much more difficult than it once did—or perhaps it has never felt easy.
This can be confusing and frustrating. Some people wonder if their body is "broken," while others worry that they are no longer attracted to their partner.
In reality, difficulty becoming aroused is one of the most common effects of sexual trauma.
Sexual arousal is not controlled by willpower alone. It depends on your brain, nervous system, emotions, hormones, blood flow, and your sense of safety all working together. When trauma has taught your brain that intimacy may be dangerous, it becomes much harder for your body to shift into a state that supports arousal.
The encouraging news is that this is often treatable.
What Is Sexual Arousal?
Sexual arousal is your body's physical response to sexual thoughts, touch, or stimulation.
It may include:
Increased blood flow to the genitals.
Natural lubrication.
Vaginal expansion.
Penile erection.
Increased sensitivity to touch.
Muscle relaxation.
A feeling of warmth or excitement.
Increased heart rate.
Arousal is a biological process that requires your nervous system to feel safe enough to relax.
If your brain is focused on survival, it becomes much more difficult for these responses to occur.
How Trauma Affects Arousal
After trauma, the brain often becomes highly sensitive to potential danger.
Instead of asking,
"Is this pleasurable?"
your nervous system may first ask,
"Am I safe?"
If the answer is uncertain, the body may automatically reduce sexual arousal in order to focus on protection rather than pleasure.
This happens without conscious choice.
Your body is trying to keep you safe.
Common Signs of Arousal Difficulties
Survivors may experience:
Feeling emotionally interested in sex but physically unresponsive.
Difficulty becoming lubricated.
Difficulty getting or maintaining an erection.
Losing arousal during intimacy.
Needing much more time to become aroused.
Feeling physically numb during sexual touch.
Feeling distracted or unable to stay present.
Becoming anxious as intimacy increases.
These experiences are common and do not mean you have failed or that your body is permanently damaged.
Arousal and Desire Are Different
Many people confuse sexual desire with sexual arousal, but they are not the same.
Sexual desire is wanting or being interested in sexual activity.
Sexual arousal is your body's physical response to sexual stimulation.
For example, someone may:
Want to have sex but struggle to become physically aroused.
Become physically aroused without feeling emotionally interested in sex.
Experience both desire and arousal.
Experience neither.
Understanding this difference can help reduce confusion and self-blame.
Why Safety Matters
The nervous system cannot fully focus on pleasure while it believes danger is nearby.
This is why survivors often notice that arousal becomes more difficult when they feel:
Rushed.
Pressured.
Anxious.
Criticized.
Disconnected from their partner.
Unsure whether they can say no.
On the other hand, arousal often improves when people experience:
Emotional safety.
Trust.
Open communication.
Patience.
Feeling respected.
Feeling in control of the pace of intimacy.
Safety is one of the strongest foundations for healthy sexual functioning.
Anxiety Can Interrupt Arousal
Even when someone deeply wants intimacy, anxiety can interrupt the body's natural sexual response.
Thoughts such as:
"What if I panic?"
"What if it hurts?"
"What if I disappoint my partner?"
"What if I have a flashback?"
"What if my body doesn't respond?"
can activate the brain's threat detection system.
Once survival mode is activated, the body naturally shifts away from sexual functioning.
This is not a lack of attraction.
It is a nervous system trying to protect you.
It's Not About Your Partner
Many partners mistakenly assume that difficulty becoming aroused means they are unattractive or unloved.
In most cases, this isn't true.
A survivor can deeply love, trust, and desire their partner while still struggling with physical arousal.
Trauma affects the nervous system—not the amount of love someone feels.
Understanding this distinction can reduce guilt for survivors and confusion for partners.
Difficulty Reaching Orgasm
Difficulty reaching orgasm is one of the most common sexual concerns experienced by survivors of sexual trauma.
For some people, orgasm becomes more difficult after the trauma. Others may have never experienced an orgasm at all. Some notice that they can reach orgasm during masturbation but not with a partner, while others may come close to orgasm only to have it disappear at the last moment.
These experiences can feel frustrating, discouraging, and isolating.
Many survivors begin to wonder:
"What's wrong with my body?"
"Will I ever orgasm again?"
"Am I broken?"
"Why can I orgasm alone but not with my partner?"
The reassuring answer is that there is nothing "wrong" with you.
Orgasm depends on your brain and nervous system feeling safe enough to fully let go. After sexual trauma, that can become much more difficult—but it is often something that can improve with healing.
How Trauma Affects Orgasm
An orgasm is not simply a physical event.
It is the result of the brain, nervous system, emotions, muscles, hormones, and body working together.
To reach orgasm, most people need to feel:
Safe.
Relaxed.
Present.
Comfortable in their body.
Able to let go of control.
After trauma, the brain may continue scanning for danger instead of allowing the body to fully relax.
Even when you consciously know you are safe, your nervous system may still be protecting you.
When the brain is focused on survival, it becomes much harder to experience pleasure.
Common Orgasm Difficulties After Trauma
Survivors may experience:
Never reaching orgasm.
Taking much longer to reach orgasm.
Feeling close to orgasm before it suddenly disappears.
Becoming distracted by anxious thoughts.
Feeling emotionally disconnected during pleasure.
Difficulty staying present.
Feeling numb during intimacy.
Avoiding orgasm because it feels vulnerable.
These experiences are common and are not signs that your body has permanently changed.
Anxiety Interrupts Pleasure
Many survivors notice that their minds become busy during intimacy.
Thoughts such as:
"Am I doing this right?"
"Does my partner think I'm attractive?"
"What if I panic?"
"What if I disappoint them?"
"What if I have a flashback?"
"Why isn't my body responding?"
These thoughts activate the brain's threat detection system.
Once the nervous system shifts into survival mode, it becomes much more difficult for the body to stay focused on pleasure.
Dissociation Can Make Orgasm Difficult
Some survivors experience dissociation during intimacy.
Instead of feeling connected to their body, they may:
Feel emotionally numb.
Feel disconnected from physical sensations.
Feel like they are observing themselves from outside their body.
Lose track of time.
Feel mentally "checked out."
Because orgasm requires awareness of physical sensations, dissociation can interrupt the body's natural sexual response.
Shame Can Block Pleasure
Many survivors carry shame about their bodies or their sexuality.
They may believe:
"I don't deserve pleasure."
"Sex isn't supposed to feel good."
"My body betrayed me."
"Something is wrong with me."
Others may feel guilty because their body experienced involuntary physical arousal during the assault.
It is important to remember:
Physical arousal is a biological reflex.
It is not consent.
It is not enjoyment.
It is not evidence that you wanted what happened.
Letting go of shame is often an important part of reclaiming sexual pleasure.
Orgasm Is Not a Performance
Many people begin viewing orgasm as something they are supposed to "achieve."
The more pressure someone feels to orgasm, the harder it often becomes.
Survivors sometimes focus so intensely on reaching orgasm that they become disconnected from the pleasure of the experience itself.
Healthy sexuality is not measured by whether or how quickly orgasm happens.
Pleasure, connection, comfort, and mutual enjoyment are equally important parts of intimacy.
Masturbation and Orgasm
Some survivors find that they are able to orgasm during masturbation but not with a partner.
This is incredibly common.
During solo sexual experiences, people often feel:
More in control.
Less pressure.
More relaxed.
Better able to communicate with their own body.
Safer.
Partnered sex introduces additional factors, including communication, vulnerability, emotional intimacy, and performance concerns, all of which can influence orgasm.
Being able to orgasm alone is actually an encouraging sign.
It demonstrates that your body is capable of experiencing pleasure.
The goal is often helping that sense of safety gradually extend into partnered intimacy.

Erectile Dysfunction After Trauma
Erectile dysfunction (ED) is one of the most common—but least discussed—effects of sexual trauma in men and people with penises.
Many survivors feel embarrassed, ashamed, or worried when they experience changes in their erections. Some assume they are no longer attracted to their partner, while others fear there is something permanently wrong with their body.
The reality is that erections depend on the brain, nervous system, emotions, hormones, blood flow, and a sense of safety all working together.
When trauma has taught the brain that intimacy may be dangerous, it becomes much more difficult for the body to shift into the relaxed state needed for an erection.
The encouraging news is that trauma-related erectile dysfunction is often treatable.
What Is Erectile Dysfunction?
Erectile dysfunction is the ongoing difficulty getting or maintaining an erection firm enough for satisfying sexual activity.
It is important to remember that everyone occasionally experiences difficulty with erections.
Stress, fatigue, illness, alcohol, medications, and relationship concerns can all affect erectile function.
Experiencing erection difficulties from time to time does not necessarily mean someone has erectile dysfunction.
However, when erections become a persistent concern, trauma may be one contributing factor.
How Trauma Affects Erections
An erection begins in the brain.
When the brain feels safe, relaxed, and sexually interested, it sends signals through the nervous system that increase blood flow to the penis.
After sexual trauma, the brain may continue scanning for danger instead of allowing the body to focus on pleasure.
The nervous system may respond by:
Increasing stress hormones.
Activating the fight, flight, freeze, or fawn response.
Increasing muscle tension.
Raising heart rate.
Keeping the body on high alert.
These survival responses interfere with the physical processes necessary for an erection.
Your body is not failing you.
It is prioritizing protection over reproduction.
Common Experiences
Survivors may notice:
Difficulty getting an erection.
Losing an erection during intimacy.
Erections that come and go unexpectedly.
Erections during masturbation but not with a partner.
Erections in some situations but not others.
Increased anxiety before sexual activity.
Fear that erection problems will happen again.
These experiences are extremely common after trauma.
Performance Anxiety and Trauma
One episode of erectile difficulty can quickly become a cycle.
A survivor may begin thinking:
"What if it happens again?"
"What if I disappoint my partner?"
"What if they think I'm not attracted to them?"
"What if they leave me?"
These anxious thoughts activate the nervous system's threat response.
Instead of relaxing, the brain begins monitoring performance.
Ironically, the harder someone tries to force an erection, the more difficult it often becomes.
This creates a cycle:
Trauma → Anxiety → Difficulty with erections → More anxiety → More erection difficulties
Fortunately, this cycle can be broken.
It's Not About Attraction
One of the biggest misconceptions about erectile dysfunction is that it means someone is no longer attracted to their partner.
In most cases, this simply isn't true.
A survivor may deeply love their partner, find them incredibly attractive, and genuinely want intimacy while still struggling with erections.
Erections are a reflection of how the nervous system is functioning—not a measure of love, desire, or masculinity.
Trauma and Shame
Many men have been taught that they should always be ready for sex and that erections should happen automatically.
These unrealistic expectations often create tremendous shame when erection difficulties occur.
Survivors may begin believing:
"I'm less of a man."
"I'm broken."
"I'm failing my partner."
"I'll never have good sex again."
These beliefs often increase anxiety, making erection difficulties even worse.
Healing begins with understanding that erectile dysfunction after trauma is a common biological response—not a personal failure.
The Role of Avoidance
Some survivors begin avoiding intimacy altogether because they fear another experience of erectile difficulty.
They may:
Avoid dating.
Turn down sexual opportunities.
Make excuses to avoid intimacy.
Pull away emotionally.
Worry constantly about sexual performance.
While avoidance may temporarily reduce anxiety, it often reinforces the nervous system's belief that sex is dangerous.
Recovery focuses on gradually rebuilding confidence rather than avoiding intimacy altogether.
Medical Causes Should Also Be Considered
Although trauma can contribute to erectile dysfunction, it is important to remember that ED can also have medical causes.
These may include:
Diabetes.
Heart disease.
High blood pressure.
Hormonal changes.
Medication side effects.
Neurological conditions.
Smoking.
Alcohol or substance use.
Sleep disorders.
Because erection difficulties can have multiple causes, it is important to speak with a healthcare provider for a complete evaluation.
Many people experience both physical and psychological contributors to erectile dysfunction.
Healing Is Possible
Trauma-related erectile dysfunction is highly treatable.
As the brain and nervous system begin recognizing that intimacy is safe again, many survivors notice improvements in:
Confidence.
Erections.
Sexual desire.
Emotional connection.
Communication with partners.
Overall sexual satisfaction.
Evidence-based treatments may include:
Eye Movement Desensitization and Reprocessing (EMDR).
Cognitive Behavioral Therapy (CBT).
Mindfulness-based approaches.
Sensate focus exercises.
Medical evaluation and treatment when appropriate.
Lifestyle changes that support cardiovascular health.
Couples therapy to improve communication and reduce pressure.
For some people, medications for erectile dysfunction may also be helpful, particularly when used alongside treatment that addresses the underlying trauma.
Recovery Is About More Than Erections
Healing isn't simply about restoring erectile function.
It's about helping your nervous system learn that intimacy can once again feel safe, connected, and enjoyable.
Many survivors discover that as they become less focused on performance and more focused on connection, erections often improve naturally.
You are not defined by your erections.
You are not less masculine because your nervous system is protecting you.
Your body has been trying to keep you safe.
With the right support, many survivors regain not only healthy erections but also confidence, intimacy, and a renewed sense of connection with themselves and their partners.

Dissociation During Sex
For many survivors of sexual trauma, one of the most confusing experiences is feeling mentally or emotionally disconnected during intimacy.
You may be physically present with your partner, yet feel as though your mind has gone somewhere else. Some survivors describe feeling numb, detached, or as though they are watching themselves from outside their body.
This experience is called dissociation, and it is one of the brain's automatic survival responses to overwhelming stress or danger.
If you experience dissociation during sex, it does not mean you don't love your partner or that you're doing something wrong.
It means your nervous system is trying to protect you.
What Is Dissociation?
Dissociation is the brain's way of creating distance from an experience that feels overwhelming.
Think of it as the brain's "emergency escape hatch."
When fighting or escaping isn't possible, the brain may disconnect from the experience to reduce emotional or physical distress.
During a traumatic event, dissociation can help someone survive.
However, after trauma, the brain may continue using dissociation during situations that remind it of the original danger—even when the person is now safe.
What Does Dissociation During Sex Feel Like?
Every survivor experiences dissociation differently.
Some people describe:
Feeling emotionally numb.
Feeling disconnected from their body.
Feeling like they are watching themselves from outside their body.
Feeling mentally "checked out."
Losing track of time.
Feeling robotic or on autopilot.
Difficulty feeling physical sensations.
Feeling disconnected from pleasure.
Difficulty remembering parts of the experience afterward.
Feeling present one moment and disconnected the next.
Some survivors remain aware that they are dissociating, while others do not recognize it until afterward.
Why Does It Happen?
Sexual intimacy naturally involves vulnerability, physical touch, and body awareness.
If those experiences were associated with danger during the trauma, the brain may automatically activate old survival strategies.
The brain is not asking:
"Do I love my partner?"
Instead, it is asking:
"Am I safe?"
If the nervous system detects even a small reminder of past trauma, dissociation may occur automatically.
This response is not a conscious decision.
It happens because your brain has learned that disconnecting helped you survive in the past.
Common Triggers
Dissociation may be triggered by:
Certain types of touch.
Specific sexual positions.
Particular smells or sounds.
Lighting or room environments.
Feeling pressured to perform.
Feeling unable to say no.
Conflict before intimacy.
Feeling emotionally vulnerable.
Medical examinations.
Memories of past trauma.
Sometimes survivors cannot identify an obvious trigger.
That does not mean the response is random.
Your brain may be responding to subtle reminders that are outside of conscious awareness.
Dissociation Is Not Rejection
Partners often misunderstand dissociation.
They may think:
"They're not attracted to me."
"They're bored."
"They don't want me."
In reality, dissociation has very little to do with attraction.
A survivor can deeply love, trust, and desire their partner while their nervous system automatically disconnects during intimacy.
Understanding dissociation can reduce unnecessary guilt for survivors and confusion for partners.
Dissociation Can Affect Pleasure
Because dissociation reduces awareness of physical sensations, it can interfere with:
Sexual arousal.
Lubrication.
Erections.
Orgasm.
Emotional connection.
Enjoyment of intimacy.
Many survivors say they feel like they are "going through the motions" rather than truly experiencing the moment.
This is not because they are choosing to disengage.
It is because the nervous system has shifted into a protective state.
Trauma-Informed Treatment
Dissociation often improves with trauma-focused treatment.
Evidence-based approaches that may help include:
Eye Movement Desensitization and Reprocessing (EMDR).
Cognitive Processing Therapy (CPT).
Somatic therapies.
Mindfulness-based interventions.
Sensorimotor Psychotherapy.
Internal Family Systems (IFS).
Grounding and nervous system regulation skills.
Many survivors also find it helpful to work with both a trauma therapist and a sex therapist, particularly if dissociation is affecting their intimate relationships.
You Can Reconnect With Your Body
One of the hardest parts of sexual trauma is feeling disconnected from your own body.
The beautiful thing about healing is that this disconnection does not have to be permanent.
Over time, your nervous system can learn that your body is no longer a place of danger—it can become a place of safety, comfort, pleasure, and connection.
Healing isn't about forcing yourself to feel something.
It's about creating enough safety that your mind and body no longer need to disconnect.
You deserve to experience intimacy while feeling fully present.
You deserve to feel connected to your body.
And with patience, support, and trauma-informed care, that is possible.
Feeling Numb or Disconnected
Many survivors of sexual trauma expect that healing will involve overwhelming emotions like sadness, fear, or anger.
Instead, many experience the opposite.
They feel...nothing.
They describe feeling emotionally numb, disconnected from themselves, or as though they are simply moving through life on autopilot.
This can be frightening.
Some survivors worry that they have become cold, uncaring, or incapable of love.
Others wonder if they are "broken" because they cannot feel joy, excitement, or even sadness the way they once did.
The truth is that emotional numbness is one of the most common effects of trauma.
It is not a personality flaw.
It is a survival response.
What Is Emotional Numbness?
Emotional numbness is a state in which emotions feel muted, distant, or absent.
Instead of experiencing the full range of human emotions, you may feel as though you're simply existing rather than truly living.
You might notice:
Feeling emotionally flat.
Difficulty feeling happiness.
Difficulty crying.
Feeling disconnected from yourself.
Feeling disconnected from other people.
Feeling like you're "going through the motions."
Losing interest in activities you once enjoyed.
Feeling emotionally empty.
Feeling detached from your own body.
For many survivors, numbness is just as distressing as anxiety or panic.
Why Does Trauma Cause Numbness?
Trauma overwhelms the brain and nervous system.
When emotions become too intense to manage, the nervous system may reduce emotional awareness to protect you.
Think of it like turning down the volume on a speaker that's become painfully loud.
The challenge is that the brain cannot easily numb only painful emotions.
When it turns down fear, grief, and shame, it often also turns down:
Joy.
Love.
Excitement.
Curiosity.
Desire.
Pleasure.
This is why many survivors say,
"I don't just feel less pain—I don't feel much of anything."
Feeling Disconnected From Your Body
Trauma can also affect your relationship with your body.
Some survivors feel as though they are living "from the neck up."
They may notice:
Feeling disconnected from physical sensations.
Difficulty noticing hunger or fullness.
Difficulty recognizing emotions.
Feeling detached during physical touch.
Feeling uncomfortable looking at their body.
Feeling like their body doesn't belong to them.
This disconnection often develops because the body became associated with danger during the traumatic experience.
The nervous system learned that disconnecting felt safer than fully experiencing what was happening.
Feeling Disconnected From Other People
Numbness doesn't only affect emotions.
It can also affect relationships.
Many survivors describe feeling emotionally distant from:
Romantic partners.
Friends.
Family members.
Children.
Coworkers.
They may love the people in their lives but struggle to feel emotionally connected to them.
This can create guilt, loneliness, and confusion.
The important thing to remember is that emotional distance is often a protective response—not a reflection of how much you care.
Numbness Can Affect Sexuality
Emotional numbness often extends into sexual experiences as well.
Survivors may notice:
Difficulty feeling pleasure.
Reduced sexual desire.
Difficulty becoming aroused.
Difficulty reaching orgasm.
Feeling emotionally absent during intimacy.
Feeling disconnected from physical touch.
This does not mean your sexuality is gone.
It means your nervous system is still prioritizing protection over connection.
As safety increases, many survivors gradually reconnect with both emotional and physical pleasure.
Numbness Is Different From Depression
Although emotional numbness can occur alongside depression, they are not the same thing.
Depression often involves persistent sadness, hopelessness, or loss of interest.
Numbness is more accurately described as the absence of emotion.
Some survivors say,
"I wish I could cry. At least then I'd know I was feeling something."
Both experiences deserve compassion and professional support.
Healing Means Reconnecting
One of the goals of trauma recovery is gently helping survivors reconnect with themselves.
Healing is not about forcing emotions to return.
It is about creating enough safety that your nervous system no longer needs to protect you by shutting emotions down.
Over time, many survivors begin noticing small changes.
They laugh more easily.
They cry when something moves them.
They feel excitement again.
They notice beauty.
They experience moments of peace.
These changes often happen gradually.
They are signs that the nervous system is learning it no longer has to stay in survival mode.
Ways to Reconnect With Yourself
Healing from emotional numbness often involves slowly rebuilding your connection with your mind and body.
Many survivors find it helpful to:
Practice grounding exercises.
Spend time in nature.
Notice physical sensations without judgment.
Engage in gentle movement such as walking or yoga.
Practice mindfulness.
Journal about thoughts and emotions.
Explore creative outlets like music or art.
Spend time with emotionally safe people.
Work with a trauma-informed therapist.
The goal isn't to force feelings.
The goal is to create enough safety that feelings naturally begin returning.
Hypersexuality as a Trauma Response
One of the most misunderstood responses to sexual trauma is hypersexuality.
Many people assume that every survivor avoids sex after trauma. While that is true for some, others experience the opposite—they may find themselves thinking about sex more often, engaging in frequent sexual activity, or feeling drawn to sexual experiences in ways that feel confusing or out of character.
This can create tremendous shame.
Many survivors ask:
"If I was traumatized, why do I want sex so much?"
"Does this mean what happened didn't affect me?"
"Does this mean I secretly wanted it?"
"Am I addicted to sex?"
The answer is no.
Hypersexuality can be one of many ways the brain and nervous system attempt to cope with overwhelming experiences.
It is not evidence that someone wanted the trauma or that they are "broken."
What Is Hypersexuality?
Hypersexuality refers to a pattern of sexual thoughts or behaviors that feel difficult to control or that are used primarily as a way of coping with emotional distress rather than for connection or pleasure.
For some survivors, this may include:
Thinking about sex frequently.
Seeking frequent sexual encounters.
Having sex despite not really wanting it.
Using sex to numb difficult emotions.
Feeling driven to seek sexual validation.
Engaging in risky sexual behaviors.
Feeling unable to stop certain sexual behaviors even when they create problems.
Feeling shame after sexual experiences.
Not every survivor experiences hypersexuality, and experiencing a high libido alone does not mean someone is hypersexual.
The key difference is why the behavior is happening.
Why Can Trauma Lead to Hypersexuality?
There is no single explanation.
Different survivors use sexual behavior for different reasons.
For some, sex becomes a way to:
Regain a sense of control.
Feel desired or accepted.
Cope with loneliness.
Escape painful emotions.
Reduce anxiety temporarily.
Feel connected to another person.
Distract themselves from intrusive memories.
Reclaim ownership of their body.
These behaviors often develop without conscious awareness.
The brain is searching for relief.
Reclaiming Control
Sexual trauma involves having control taken away.
Some survivors later choose sexual experiences as a way of reclaiming that control.
They may think:
"This time I'm choosing."
"This time I'm in charge."
"This time no one is forcing me."
For many survivors, this can be an important part of healing.
For others, however, sexual behavior may begin to feel compulsive or disconnected from their actual desires.
The goal is not to judge the behavior.
The goal is to understand what need the behavior is trying to meet.
Seeking Validation
Trauma can profoundly affect self-worth.
Some survivors begin seeking validation through sex because it temporarily provides feelings of:
Being wanted.
Being attractive.
Being accepted.
Feeling connected.
Feeling valued.
These feelings are real.
The difficulty is that they are often temporary.
Once the sexual experience ends, feelings of shame, loneliness, or emptiness may return.
This can create a cycle in which someone continues seeking sexual experiences in hopes of feeling better.
Coping With Emotional Pain
For some survivors, sex becomes a coping strategy.
Just as some people cope through alcohol, food, work, or excessive exercise, others cope through sexual behavior.
Sex may temporarily reduce:
Anxiety.
Loneliness.
Emotional numbness.
Stress.
Intrusive thoughts.
Feelings of worthlessness.
The problem is that the relief often doesn't last.
Without addressing the underlying trauma, the emotional pain usually returns.
Hypersexuality Does Not Mean You Enjoyed the Trauma
One of the most damaging myths survivors tell themselves is:
"If I'm hypersexual now, maybe what happened wasn't really traumatic."
This is false.
How you respond after trauma says nothing about whether the trauma occurred or how much it affected you.
Avoiding sex, seeking sex, losing desire, or experiencing increased desire are all possible trauma responses.
There is no "correct" way for a survivor to respond.
Trauma Can Affect Sexual Boundaries
Some survivors notice that they have difficulty recognizing or honoring their own boundaries after trauma.
They may:
Agree to sex they don't actually want.
Have difficulty saying no.
Prioritize someone else's needs over their own.
Feel guilty setting limits.
Confuse compliance with desire.
These patterns often develop because trauma disrupted the survivor's sense of safety, autonomy, or consent.
Healing includes learning that your needs, comfort, and boundaries matter.
Moving From Survival to Choice
One of the goals of healing is helping survivors distinguish between sex that is motivated by survival and sex that is motivated by genuine desire.
A helpful question is not:
"How often am I having sex?"
Instead, ask:
Am I choosing this freely?
Do I actually want this?
Do I feel emotionally safe?
Am I seeking connection or escaping pain?
Will this choice leave me feeling more connected to myself?
The frequency of sexual activity does not determine whether it is healthy.
The presence of choice, consent, safety, and authenticity does.
Healing Your Relationship With Sexuality
Healing is not about eliminating sexual desire.
Nor is it about judging yourself for the ways you've coped.
Healing is about creating a relationship with sexuality that feels:
Safe.
Consensual.
Authentic.
Enjoyable.
Connected.
Free from shame.
Guided by your own values.
Many survivors find that as they process their trauma, their sexual behaviors become less driven by survival and more guided by genuine desire.

Feeling Guilty for Enjoying Sex Again
For many survivors, one of the most unexpected parts of healing is not learning how to enjoy sex again—it's giving themselves permission to enjoy it.
As healing begins, some survivors notice moments of desire, pleasure, or even excitement during intimacy. Instead of feeling relieved, they feel guilty.
They may wonder:
"Am I allowed to enjoy sex after what happened?"
"Does enjoying sex mean I'm forgetting the trauma?"
"Does this mean it wasn't really that bad?"
"Am I betraying myself by moving on?"
"How can I enjoy something that was used to hurt me?"
These questions are incredibly common.
The answer is simple:
You are allowed to heal.
And you are allowed to experience pleasure again.
Healing Does Not Erase What Happened
One of the biggest fears many survivors have is that enjoying sex again somehow minimizes the trauma.
It doesn't.
Healing does not erase the past.
It does not excuse the person who harmed you.
It does not mean the trauma wasn't real.
Healing simply means that the trauma no longer gets to decide every part of your future.
You can honor what happened while also allowing yourself to experience happiness, love, and pleasure.
The two can exist together.
Pleasure Is Not Betrayal
Some survivors feel as though enjoying sex is somehow betraying the version of themselves who was hurt.
They may believe:
"I shouldn't enjoy this."
"I don't deserve pleasure."
"I should still be suffering."
"If I heal, people will think I'm over it."
These beliefs often come from shame—not truth.
The person responsible for the trauma took away your choice.
Healing is about giving that choice back to yourself.
Choosing pleasure is not betrayal.
It is reclaiming something that always belonged to you.
Your Body Deserves Joy
Sexual trauma can make survivors feel disconnected from their bodies.
Some begin seeing their body only as a place where something terrible happened.
But your body is so much more than what happened to it.
Your body deserves:
Safety.
Kindness.
Respect.
Care.
Comfort.
Affection.
Pleasure.
The trauma does not own your body.
The person who hurt you does not own your sexuality.
You do.
It's Okay If Pleasure Feels Complicated
Healing is rarely simple.
Some survivors feel both pleasure and sadness during the same experience.
Others notice that moments of intimacy bring tears, fear, relief, gratitude, or grief all at once.
These mixed emotions are completely normal.
You might:
Enjoy physical touch while feeling emotionally vulnerable.
Feel safe with your partner but still have moments of fear.
Experience pleasure followed by unexpected sadness.
Feel proud of your healing while grieving what was taken from you.
Healing often involves holding more than one emotion at the same time.
You Do Not Need to Earn Pleasure
Many survivors believe they must be "fully healed" before they deserve intimacy.
They tell themselves:
"I'm not ready."
"I'm too damaged."
"I need to fix myself first."
The reality is that healing often happens within safe, respectful, connected relationships.
You do not have to become a perfect version of yourself before you deserve love or pleasure.
You deserve both simply because you are human.
Reclaiming Your Sexuality
Healing is not about returning to the person you were before the trauma.
Many survivors discover that they are creating something entirely new.
They begin building a sexuality that is based on:
Choice.
Consent.
Curiosity.
Communication.
Safety.
Mutual respect.
Pleasure.
Authenticity.
Instead of asking,
"Can I ever go back?"
many survivors eventually begin asking,
"What kind of sexual relationship do I want to create moving forward?"
That question shifts the focus from the past to the future.
Healing Can Include Joy
Sometimes survivors worry that if they laugh, fall in love, or enjoy sex again, it means they are leaving the trauma behind.
In reality, healing allows you to carry your story differently.
The trauma may always be part of your life story.
It does not have to be the entire story.
You can remember what happened and still:
Fall in love.
Trust someone.
Feel desire.
Experience orgasm.
Enjoy intimacy.
Laugh freely.
Feel connected to your body.
Build a healthy relationship.
Healing makes room for both remembrance and hope.
Giving Yourself Permission
If no one has ever told you this before, hear it now:
You have permission to enjoy your body again.
You have permission to laugh during sex.
You have permission to feel desire.
You have permission to experience pleasure.
You have permission to say yes when you want to—and no when you don't.
You have permission to heal.
The person who hurt you took enough from you already.
You do not have to give them your future, too.

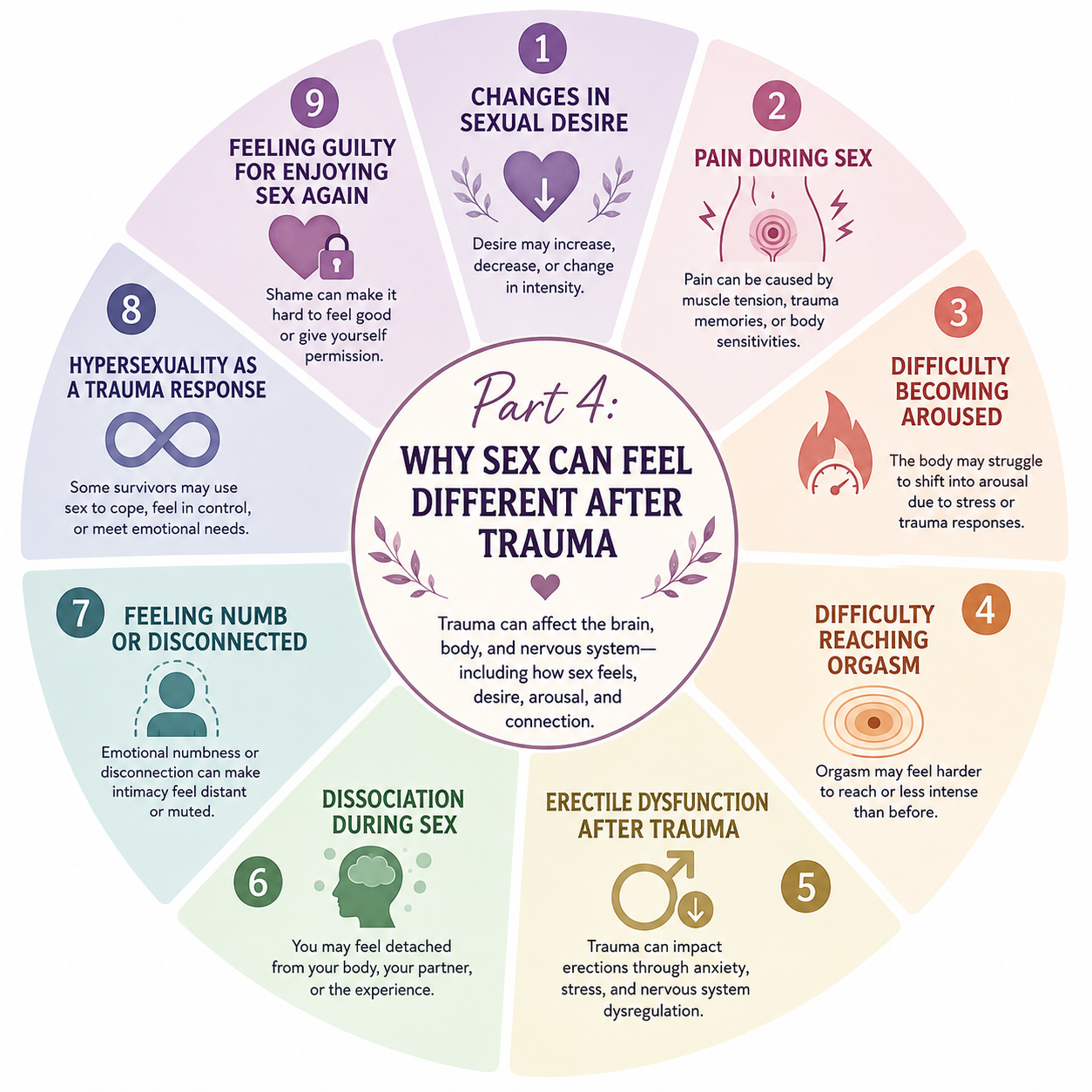
Part 5: Understanding Triggers
What Is a Trigger?
One of the most frustrating parts of healing from sexual trauma is feeling like the trauma is happening all over again—even when you know you're safe.
A smell, a sound, a certain touch, or even a seemingly ordinary situation can suddenly trigger intense fear, anxiety, panic, or emotional distress.
These experiences are called triggers.
Triggers are one of the most common effects of trauma, and understanding them can be incredibly empowering.
A trigger is not a sign that you're "going backward."
It is a sign that your brain and nervous system are trying to protect you.
What Is a Trauma Trigger?
A trauma trigger is anything that reminds your brain or body of a past traumatic experience and activates your nervous system's survival response.
Triggers can cause your brain to react as though the danger is happening again—even when you are completely safe in the present.
This happens because traumatic memories are often stored differently than ordinary memories.
Instead of feeling like something that happened in the past, trauma reminders can feel immediate and intensely real.
Triggers Can Be Obvious or Subtle
Some triggers are easy to recognize.
Others seem completely unexpected.
Common triggers include:
Certain smells or perfumes.
Specific songs or music.
Certain words or phrases.
Raised voices.
Physical touch.
Sexual intimacy.
Medical examinations.
Certain locations.
Particular dates or anniversaries.
Seeing someone who resembles the person who harmed you.
Movies, television shows, or news stories about sexual violence.
Other triggers may be much more subtle.
For example, a certain season, the lighting in a room, a facial expression, or even a particular type of clothing may activate memories without you realizing why.
Sometimes the brain notices patterns long before the conscious mind does.
Emotional Triggers
Not all triggers come from things you see or hear.
Sometimes emotions themselves become triggers.
For example, feeling:
Vulnerable.
Rejected.
Powerless.
Trapped.
Embarrassed.
Ashamed.
Alone.
may activate memories of the trauma.
Your brain isn't reacting to the emotion itself.
It's reacting to what that emotion once meant during the traumatic experience.
Body Triggers
The body also remembers trauma.
Certain physical sensations may activate the nervous system, including:
Increased heart rate.
Muscle tension.
Heavy breathing.
Pain.
Feeling cornered.
A racing heartbeat during exercise.
Certain sexual sensations.
Pelvic examinations.
Medical procedures.
Sometimes survivors experience a trigger without any external reminder at all.
Instead, the body itself becomes the reminder.
Why Triggers Feel So Intense
When the brain detects a reminder of trauma, the amygdala—the brain's alarm system—responds immediately.
Before your thinking brain has time to evaluate whether you're actually safe, your nervous system may activate the fight, flight, freeze, or fawn response.
This can cause:
Panic.
Fear.
Anxiety.
Dissociation.
Emotional numbness.
Muscle tension.
Rapid heartbeat.
Crying.
Feeling overwhelmed.
Wanting to escape.
This response happens automatically.
It is not a conscious decision.
A Trigger Is Not the Same as Danger
One of the most important parts of trauma recovery is learning the difference between a trigger and a current threat.
A trigger is a reminder of something dangerous that happened in the past.
A current threat is something dangerous happening right now.
After trauma, the brain sometimes struggles to tell the difference.
This is why survivors often say:
"I know I'm safe, but my body doesn't."
Healing helps the brain and nervous system recognize that the traumatic event is over—even when reminders appear.
Triggers Can Change Over Time
Triggers are not permanent.
Some become less intense as healing progresses.
Others disappear completely.
You may also notice new triggers as you process different parts of your trauma.
This is a normal part of recovery.
Healing is not measured by never being triggered.
It is measured by how quickly your nervous system is able to recognize that you are safe again.
Avoiding Every Trigger Isn't the Goal
Many survivors try to avoid anything that reminds them of the trauma.
While this can provide temporary relief, avoiding every trigger often causes the brain to become even more sensitive over time.
Instead, trauma treatment focuses on helping your nervous system gradually learn that reminders are not the same as danger.
This process should happen slowly and safely, often with the guidance of a trauma-informed therapist.
Healing isn't about forcing yourself into triggering situations.
It's about expanding your sense of safety so that reminders lose their power over time.
Common Sexual Trauma Triggers
No two survivors have the exact same triggers.
Something that causes one person to feel overwhelmed may have no effect on someone else. Likewise, a trigger that feels incredibly intense today may become much less distressing as healing progresses.
Triggers are deeply personal because they are based on your unique experiences, memories, and nervous system.
Understanding your triggers is not about avoiding life.
It is about recognizing what your brain has learned to associate with danger so you can respond with self-compassion instead of self-blame.
Below are some of the most common triggers reported by survivors of sexual trauma.
Physical Touch
Touch is one of the most common trauma triggers.
Even safe, loving touch can activate the nervous system if it resembles sensations experienced during the trauma.
Common touch-related triggers include:
Unexpected touch.
Being hugged without warning.
Someone standing very close.
Touching certain parts of the body.
Being restrained or held.
Tickling.
Back rubs or massages.
Affectionate touch during stressful moments.
Remember, your body may react automatically before your conscious mind realizes you're safe.
Sexual Intimacy
For many survivors, sexual experiences themselves become triggers.
This does not mean sex is unsafe.
It means the brain has learned to associate certain aspects of intimacy with past danger.
Possible triggers include:
Kissing.
Undressing.
Nudity.
Certain sexual positions.
Oral sex.
Penetration.
Specific sexual acts.
Being touched in certain ways.
Feeling pressure to have sex.
Feeling unable to stop or slow down.
Some survivors notice they feel safe at the beginning of intimacy but become triggered as vulnerability increases.
Smells
Smell is one of the strongest memory triggers because the brain regions responsible for smell are closely connected to areas involved in emotion and memory.
Common scent-related triggers include:
Cologne or perfume.
Alcohol.
Cigarette smoke.
Laundry detergent.
Body wash or shampoo.
Breath odors.
Hospitals or medical disinfectants.
Certain foods.
Sometimes a smell can trigger an emotional reaction before you consciously recognize what you're smelling.
Sounds
Certain sounds can quickly activate the nervous system.
Examples include:
Raised voices.
Yelling.
Footsteps behind you.
Doors slamming.
Keys jingling.
Heavy breathing.
Specific songs.
Television scenes.
Sirens.
Laughter that resembles someone's voice.
Music can be particularly powerful because it often becomes linked with specific memories.
Places
Returning to certain locations can trigger powerful emotional responses.
Examples include:
A particular neighborhood.
Schools or college campuses.
A bedroom.
Hotels.
Bars or clubs.
Parking lots.
Medical offices.
Public transportation.
Workplaces.
Sometimes simply driving past a familiar location can activate memories.
Medical Appointments
Many survivors find healthcare visits particularly challenging.
Common triggers include:
Pelvic examinations.
Prostate exams.
Pap smears.
STI testing.
Pregnancy-related care.
Being asked to undress.
Physical examinations.
Dental procedures involving limited control.
Feeling physically vulnerable.
Trauma-informed healthcare providers can often help make these experiences feel safer.
Clothing
Certain clothing or fabrics may trigger memories.
Examples include:
Wearing similar clothing to what you wore during the trauma.
Seeing someone dressed similarly to the person who harmed you.
Hospital gowns.
Tight clothing.
Certain uniforms.
Specific jewelry or accessories.
Time and Dates
The body sometimes remembers important dates even when the mind does not consciously think about them.
You may notice increased symptoms around:
The anniversary of the trauma.
Holidays.
Birthdays.
Certain seasons.
Particular times of day.
Weather that resembles the day of the trauma.
This is sometimes called an anniversary reaction, and it is a common trauma response.
Conflict
Arguments and conflict can activate survival responses even when the disagreement is healthy.
Triggers may include:
Raised voices.
Criticism.
Feeling misunderstood.
Feeling trapped during an argument.
Someone blocking your exit.
Feeling powerless.
Someone refusing to listen.
For some survivors, conflict immediately activates the fight, flight, freeze, or fawn response.
Loss of Control
Many survivors become especially sensitive to situations where they feel they have little control.
Examples include:
Feeling pressured to make a decision.
Being interrupted.
Someone making decisions without asking.
Being physically blocked.
Feeling trapped in traffic.
Being unable to leave a room.
Crowded spaces.
Airplane travel.
Medical procedures.
Having choices often helps the nervous system feel safer.
Body Sensations
Sometimes the trigger comes from within your own body.
Examples include:
A racing heart.
Sweating.
Muscle tension.
Pelvic pain.
Rapid breathing.
Feeling physically aroused.
Fatigue.
Certain hormonal changes.
Because these sensations resemble what happened during the trauma, the brain may mistakenly interpret them as signs of danger.
Pregnancy and Parenting
Some survivors find that pregnancy, childbirth, breastfeeding, or parenting activate memories they did not expect.
Possible triggers include:
Prenatal medical exams.
Labor and delivery.
Breastfeeding.
Diaper changes.
Teaching children about body safety.
Watching children reach the age they were when they experienced trauma.
These reactions are more common than many survivors realize.
Seeing the Person Who Harmed You
For survivors who encounter the person responsible for the trauma—or someone who closely resembles them—the nervous system may react immediately.
Even seeing a photograph, hearing their name, or receiving a message from them can activate intense emotions.
Emotional Triggers
Not every trigger is connected to a place or object.
Certain emotional experiences can also activate trauma responses, including:
Feeling rejected.
Feeling abandoned.
Feeling powerless.
Feeling embarrassed.
Feeling ashamed.
Feeling judged.
Feeling helpless.
Feeling ignored.
Feeling lonely.
Sometimes the emotion itself is what reminds the brain of the trauma.
Your Triggers Are Unique
This list is not meant to suggest that you will experience every trigger.
You may have triggers that are not listed here, or you may never experience many of the examples above.
There is no "right" or "wrong" trigger.
Your brain created these associations in an effort to protect you.
Understanding your unique triggers can help you respond with curiosity instead of self-criticism.

Trigger vs. Actual Danger
One of the most important goals of trauma recovery is learning to recognize the difference between a trigger and actual danger.
After sexual trauma, the brain often becomes extremely good at detecting anything that resembles the traumatic experience. This is a normal survival response. Your brain is trying to prevent you from ever being hurt in the same way again.
The challenge is that the brain sometimes mistakes reminders of the past for threats in the present.
As a result, your body may react as though you are in danger—even when you are completely safe.
Learning this difference is one of the most powerful steps in healing.
What Is a Trigger?
A trigger is a reminder of a past traumatic experience that activates your brain's survival response.
A trigger can be:
A smell.
A sound.
A place.
A person.
Physical touch.
A medical appointment.
Sexual intimacy.
A certain emotion.
A body sensation.
A specific date or anniversary.
Triggers activate memories stored in the brain and nervous system.
They remind your body of what happened.
But they are not the trauma itself.
What Is Actual Danger?
Actual danger is a situation in which there is a real, immediate threat to your safety.
Examples include:
Someone threatening or assaulting you.
Being physically unsafe.
A medical emergency.
Being trapped in an abusive situation.
Experiencing ongoing violence or coercion.
In these situations, your survival response is doing exactly what it is supposed to do—helping protect you.
The goal of trauma healing is not to eliminate your ability to recognize real danger.
It is to help your brain become more accurate at distinguishing between the past and the present.
Why the Brain Gets Confused
During trauma, the brain prioritizes survival over detailed memory.
Instead of storing the experience as:
"This happened years ago."
the brain often stores pieces of the experience as:
Images.
Sounds.
Smells.
Physical sensations.
Emotions.
Body memories.
When one of these reminders appears, the amygdala—the brain's alarm system—may sound the alarm before the thinking part of the brain has time to evaluate the situation.
Your nervous system reacts first.
Your logical brain catches up later.
This is why so many survivors say:
"I knew I was safe, but my body didn't believe it."
Your Body Cannot Tell Time
One of the most helpful ways to understand trauma is this:
Your body remembers the past as if it is happening in the present.
When you are triggered, your nervous system isn't choosing to overreact.
It is responding to old information.
Your brain is saying,
"This feels like what hurt us before. Protect us."
That response once helped you survive.
Now it simply needs updating.
Common Examples
Imagine someone who was assaulted while smelling a particular cologne.
Years later, they walk into an elevator and smell that same cologne.
Immediately they notice:
Their heart races.
Their stomach tightens.
Their breathing becomes shallow.
They feel panicked.
They want to leave.
The cologne is the trigger.
The elevator is not the danger.
Their nervous system has confused a reminder with a current threat.
Here's another example.
A survivor's partner reaches over unexpectedly to touch their shoulder.
The survivor jumps, freezes, or pulls away.
Their loving partner is not the danger.
The unexpected touch is the trigger because it resembles something their nervous system once experienced during the trauma.
How to Tell the Difference
When you notice yourself becoming triggered, gently ask yourself:
Am I safe right now?
Is this happening today, or is it reminding me of something from the past?
What is my nervous system reacting to?
What evidence tells me I am safe in this moment?
What would I tell a friend in this situation?
These questions help activate the thinking part of the brain and remind your nervous system that the present is different from the past.
Grounding Yourself in the Present
When you're triggered, your nervous system may need reminders that you are here, now—not back in the traumatic experience.
Grounding techniques can help by bringing your attention back to the present moment.
Some examples include:
Naming five things you can see.
Feeling your feet on the floor.
Taking slow, steady breaths.
Holding a comforting object.
Looking around the room and identifying signs of safety.
Saying today's date out loud.
Reminding yourself:
"I'm safe."
"This is a memory, not the trauma."
"The danger has passed."
Grounding doesn't erase the trigger.
It helps your brain reconnect with the present.
Healing Helps the Brain Update
One of the goals of trauma therapy is helping the brain recognize that the traumatic event is over.
Evidence-based treatments such as Eye Movement Desensitization and Reprocessing (EMDR) and other trauma-focused therapies help the brain process memories differently.
Over time, survivors often notice that:
Triggers become less intense.
Recovery happens more quickly.
The body no longer reacts as strongly.
They feel more confident recognizing when they are truly safe.
Healing isn't about forgetting what happened.
It's about teaching your brain that what happened belongs in the past—not the present.
You Can Trust Yourself Again
Many survivors lose confidence in their ability to judge whether they are safe.
That is understandable.
Trauma can make the world feel unpredictable.
But healing helps rebuild that trust.
Over time, your brain becomes better at distinguishing between a memory and a real threat.
You begin responding to today's reality instead of yesterday's danger.
That doesn't mean you'll never be triggered again.
It means your triggers no longer get to decide how you live your life.

Managing Triggers
Learning to manage triggers is one of the most important parts of recovering from sexual trauma.
Many survivors believe that healing means never being triggered again.
In reality, healing is not about eliminating every trigger.
It is about helping your brain and nervous system recognize that you are safe now.
Over time, triggers often become less intense, happen less frequently, and feel much more manageable.
You may still notice reminders of your trauma, but they no longer have the same power over your thoughts, emotions, or body.
Managing triggers is about responding with compassion instead of fear.
Step 1: Notice That You Have Been Triggered
The first step is recognizing when your nervous system has shifted into survival mode.
Many survivors don't immediately realize they have been triggered.
Instead, they simply notice that they suddenly feel:
Anxious.
Irritable.
Numb.
Panicked.
Angry.
Overwhelmed.
Frozen.
Like they need to leave.
Like they are no longer present.
Learning to recognize these early signs gives you the opportunity to respond before the trigger becomes overwhelming.
Step 2: Name What Is Happening
Once you recognize that you have been triggered, gently remind yourself:
"I'm having a trauma response."
Or:
"This is a trigger—not a current danger."
Naming your experience helps activate the thinking part of your brain and reminds your nervous system that what you're experiencing is a memory, not an emergency.
Step 3: Ground Yourself in the Present
Triggers pull your nervous system into the past.
Grounding helps bring you back to the present.
Some grounding techniques include:
The 5-4-3-2-1 Technique
Notice:
5 things you can see.
4 things you can touch.
3 things you can hear.
2 things you can smell.
1 thing you can taste.
This simple exercise reminds your brain that you are here—not back in the traumatic experience.
Focus on Your Breathing
When we're triggered, our breathing often becomes shallow and rapid.
Try slowing your breath.
For example:
Inhale for four seconds.
Hold for two seconds.
Exhale for six seconds.
A longer exhale signals to your nervous system that it can begin to relax.
Step 4: Orient Yourself to Safety
Take a slow look around the room.
Ask yourself:
Where am I?
What year is it?
Who is with me?
Am I safe right now?
Is there any immediate danger?
Your eyes are one of the fastest ways to communicate safety to your nervous system.
Simply looking around your environment and noticing that nothing threatening is happening can help your brain shift out of survival mode.
Step 5: Remind Yourself of the Truth
Trauma often causes the brain to believe that the past is happening again.
Gentle reminders can help update your nervous system.
You might say:
"The trauma is over."
"I survived."
"I am safe right now."
"This feeling will pass."
"My body is remembering the past."
"I don't have to protect myself from something that isn't happening."
These statements are not about convincing yourself.
They are about helping your brain reconnect with reality.
Step 6: Move Your Body
Trauma activates the body's survival response.
Gentle movement can help release some of that activation.
Helpful activities include:
Walking.
Stretching.
Yoga.
Shaking out your arms and legs.
Deep breathing with movement.
Dancing.
Progressive muscle relaxation.
Movement reminds your nervous system that it is no longer trapped.
Step 7: Practice Self-Compassion
Many survivors become frustrated when they are triggered.
They think:
"I should be over this."
"What's wrong with me?"
"I'm failing."
Instead, try asking:
"What does my nervous system need right now?"
Perhaps it needs:
Rest.
Water.
A supportive friend.
Quiet.
Fresh air.
Comfort.
Reassurance.
Healing grows through compassion, not criticism.
Step 8: Communicate With Safe People
If you have a trusted partner, friend, or family member, let them know what helps when you're triggered.
For example, you might say:
"If I become quiet, please give me a few minutes."
"Please ask before touching me."
"Remind me to breathe."
"Help me remember where I am."
"Please stay with me unless I ask for space."
Healthy communication allows supportive people to respond in ways that help your nervous system feel safer.
Step 9: Learn Your Patterns
Many survivors begin noticing that their triggers follow patterns.
You may find it helpful to keep a journal of:
What happened before the trigger?
What thoughts showed up?
What emotions did you notice?
How did your body react?
What helped you recover?
Over time, these patterns can help you better understand your nervous system and prepare for situations that may be challenging.
Step 10: Seek Trauma-Informed Treatment
You do not have to manage triggers alone.
Working with a trauma-informed therapist can help your brain process traumatic memories so they become less distressing over time.
Evidence-based treatments such as:
Eye Movement Desensitization and Reprocessing (EMDR)
Cognitive Processing Therapy (CPT)
Trauma-Focused Cognitive Behavioral Therapy (TF-CBT)
Prolonged Exposure Therapy (PE)
Somatic therapies
Mindfulness-based therapies
have been shown to reduce the intensity and frequency of trauma triggers.
The goal of therapy is not to erase your memories.
It is to help your nervous system recognize that the danger has passed.
Progress Is Measured Differently Than You Think
Many survivors believe progress means never getting triggered.
A healthier way to measure progress is to ask:
Do I recognize triggers more quickly?
Do I recover faster than I used to?
Am I less afraid of my reactions?
Am I treating myself with more compassion?
Do I have tools that help me feel safe again?
If the answer is yes, healing is happening.
Healing Is Possible
Every time your nervous system experiences safety after a trigger, it learns something new.
It learns that not every reminder leads to danger.
It learns that the trauma is over.
It learns that you survived.
These repeated experiences gradually help the brain rewrite old survival patterns.
Healing doesn't happen because you stop having triggers.
Healing happens because triggers stop controlling your life.
With time, practice, and trauma-informed support, your brain can learn that the present is different from the past—and that you are safe enough to move forward.

Part 6: Dissociation
What Is Dissociation?
One of the most confusing experiences after sexual trauma is feeling disconnected from yourself, your body, or the world around you.
Many survivors describe feeling like they are watching life instead of living it. Others say they feel emotionally numb, disconnected from their bodies, or as though they are on "autopilot."
These experiences can be frightening, especially if you don't understand why they are happening.
The good news is that dissociation is a well-known trauma response.
It is not a sign that you are "going crazy."
It is your brain's way of protecting you during overwhelming experiences.
Understanding dissociation is often the first step toward reducing the fear and confusion surrounding it.
What Is Dissociation?
Dissociation is a temporary disconnection between your thoughts, emotions, memories, body, or surroundings.
Think of it as the brain's emergency safety system.
When an experience feels too overwhelming to fully process, the brain may create distance from it in order to help you survive.
For many survivors, dissociation was incredibly protective during the trauma.
The problem is that the brain may continue using this same strategy long after the danger has ended.
Dissociation Is a Survival Response
Most people have heard of the fight, flight, freeze, and fawn responses.
Dissociation is another survival response.
When fighting or escaping is impossible, the brain sometimes protects itself by disconnecting from what is happening.
This may reduce emotional pain, physical pain, or awareness of the traumatic experience.
It is not a conscious decision.
Your nervous system makes this choice automatically.
Common Signs of Dissociation
Dissociation can look different for everyone.
Some survivors experience:
Feeling emotionally numb.
Feeling disconnected from your body.
Feeling like you're watching yourself from outside your body.
Feeling like you're living in a dream.
Feeling mentally "checked out."
Losing track of time.
Having difficulty remembering parts of conversations or events.
Feeling disconnected from your emotions.
Feeling detached from the people around you.
Feeling like the world isn't quite real.
Some people experience dissociation only during stressful situations.
Others notice it happens throughout the day without realizing it.
Dissociation Exists on a Spectrum
Not all dissociation is severe.
In fact, everyone experiences mild dissociation from time to time.
For example, you may have:
Driven somewhere and not remembered part of the drive.
Become so absorbed in a movie or book that you lost awareness of your surroundings.
Daydreamed during a meeting or class.
Missed part of a conversation because your mind wandered.
These everyday experiences are normal.
Trauma-related dissociation is different because it is driven by your nervous system's attempt to protect you from overwhelming distress.
Why Does Dissociation Continue After Trauma?
After sexual trauma, the brain becomes highly sensitive to anything that resembles the original experience.
If the nervous system detects danger—or even something that reminds it of danger—it may automatically use dissociation again.
The brain is trying to help.
It simply hasn't learned that the trauma is over.
Instead of asking,
"Am I safe?"
the nervous system assumes,
"This feels familiar. I need to protect us."
What Does Dissociation Feel Like?
Survivors often describe dissociation in different ways.
Some say:
"I feel like I'm watching my life instead of living it."
"Everything feels foggy."
"I know I'm here, but I don't feel here."
"It feels like my body doesn't belong to me."
"Sometimes I lose time."
"I can't connect with my emotions."
"I feel empty."
"Nothing feels real."
These experiences can be unsettling, but they are common among trauma survivors.
Dissociation Is Not Weakness
Many survivors feel embarrassed by dissociation.
They may think:
"Why can't I just stay present?"
"What's wrong with me?"
"I should be stronger."
The reality is that dissociation reflects how powerfully your brain worked to keep you alive.
It developed because your nervous system believed there were no other options.
It is not a character flaw.
It is not attention-seeking.
It is not something you are choosing to do.
It is a biological survival response.
Dissociation Can Affect Daily Life
When dissociation continues after trauma, it can affect many areas of life.
Some survivors notice difficulty with:
Concentration.
Memory.
Work or school.
Relationships.
Parenting.
Driving.
Emotional connection.
Sexual intimacy.
Decision-making.
These challenges can feel frustrating, but they often improve as the underlying trauma is treated.

Why Dissociation Happens
Many survivors wonder why their brain seems to "shut down" during stressful situations.
They may ask:
"Why do I disappear mentally?"
"Why can't I stay present?"
"Why do I feel numb instead of emotional?"
"Why can't I remember parts of what happened?"
The answer is simple:
Your brain is trying to protect you.
Dissociation is not a flaw or a sign that something is wrong with you. It is one of the brain's most powerful survival strategies.
When an experience feels too overwhelming to fight, escape, or fully process, the brain sometimes responds by disconnecting.
This response helped many survivors survive the trauma.
Your Brain's Number One Job
The brain has one primary goal:
Keep you alive.
It is not designed to make you happy.
It is not designed to help you enjoy life.
Its first priority is survival.
When your brain believes you are in danger, it immediately activates survival responses.
Sometimes that means:
Fighting.
Running away.
Freezing.
Appeasing the threat.
But when none of those options seem possible, the brain may choose something else.
It disconnects.
When Escape Isn't Possible
Imagine a child experiencing abuse by someone they depend on.
They cannot fight.
They cannot leave.
They cannot call for help.
Their nervous system recognizes that escape isn't possible.
So instead of trying to change the situation, the brain changes their experience of the situation.
It creates emotional distance.
It reduces awareness.
It disconnects from pain.
This isn't giving up.
It's surviving.
The Brain's Emergency Escape Hatch
You can think of dissociation as your brain's emergency escape hatch.
If your body cannot leave the situation, your mind tries to.
This may look like:
Feeling emotionally numb.
Feeling detached from your body.
Feeling like you're watching everything happen from outside yourself.
Feeling unreal.
Losing awareness of time.
Having difficulty remembering parts of the event.
These responses reduce the emotional intensity of an experience that feels impossible to endure.
The Nervous System Learns Patterns
The brain is incredibly good at learning.
If dissociation helped you survive once, your nervous system remembers.
Later in life, situations that resemble the trauma may automatically activate the same response—even when you're no longer in danger.
Your nervous system thinks:
"This worked before. I'll use it again."
The brain isn't trying to make life difficult.
It's repeating the strategy that once kept you alive.
Your Body Doesn't Know the Trauma Is Over
One of the biggest challenges after trauma is that the nervous system often continues responding as though the danger is still happening.
Your logical brain may know:
"I am safe."
But your survival brain may still believe:
"I need to protect us."
That is why dissociation can happen during:
Arguments.
Medical appointments.
Sexual intimacy.
Loud noises.
Conflict.
Feeling trapped.
Emotional vulnerability.
Physical touch.
Your body is reacting to what feels familiar—not to what is actually happening today.
Dissociation Is an Automatic Response
Many survivors blame themselves because they cannot control when dissociation happens.
The truth is:
You are not choosing to dissociate.
It happens automatically.
Just like you don't consciously decide to blink when something flies toward your face, you don't consciously decide to dissociate.
Your nervous system acts before your thinking brain has time to respond.
This is why trying to "just stay present" often doesn't work.
The nervous system must first learn that it is safe.
Why Some People Dissociate More Than Others
Not everyone responds to trauma in the same way.
Many factors influence whether someone develops dissociation, including:
Age at the time of the trauma.
How long the trauma lasted.
Whether the trauma happened repeatedly.
Whether the person could escape.
Whether there was a trusted adult or safe person available.
Individual differences in the nervous system.
Children are particularly likely to develop dissociation because they have fewer options for protecting themselves.
Dissociation Was Adaptive
It is important to remember that dissociation developed for a reason.
Without it, many survivors may have experienced even greater emotional suffering during the trauma.
In that moment, dissociation was not the problem.
It was the solution.
The challenge is that the brain continues using that solution long after it is no longer needed.
Healing Means Teaching the Brain a New Response
Recovery is not about forcing yourself to stop dissociating.
It is about helping your nervous system learn that it has new options.
Over time, your brain begins replacing automatic disconnection with:
Awareness.
Grounding.
Emotional regulation.
Connection.
Choice.
Safety.
Evidence-based treatments such as Eye Movement Desensitization and Reprocessing (EMDR), somatic therapies, Internal Family Systems (IFS), and other trauma-informed approaches help the brain update these old survival patterns.
As the traumatic memories become integrated, the nervous system no longer needs to disconnect so quickly.
Your Brain Is Trying to Protect You
Many survivors spend years asking,
"What's wrong with me?"
A more healing question is:
"What was my brain trying to protect me from?"
That small shift changes everything.
Instead of seeing dissociation as a weakness, you begin seeing it for what it truly is:
A remarkable survival strategy developed by a brain that was doing everything it could to keep you alive.
Now your brain can learn something new.
It can learn that the trauma is over.
It can learn that you are safe.
And little by little, it can learn that it no longer has to disconnect in order to survive.
Signs of Dissociation
Dissociation can look very different from person to person.
Some survivors recognize it immediately.
Others live with dissociation for years before realizing what they are experiencing has a name.
Because dissociation is designed to help you disconnect from overwhelming experiences, it can sometimes be difficult to recognize while it is happening.
Many survivors simply think,
"This is just who I am."
In reality, many of these experiences are common trauma responses.
Learning to recognize the signs of dissociation is an important step toward healing.
Emotional Signs
Many survivors notice changes in their emotions.
You may experience:
Feeling emotionally numb.
Feeling disconnected from your emotions.
Difficulty crying, even when you want to.
Feeling emotionally flat.
Feeling detached from people you care about.
Feeling like you're watching life instead of living it.
Difficulty experiencing joy or excitement.
Feeling emotionally "shut down."
These experiences are not signs that you don't care.
They are signs that your nervous system may be protecting you from emotional overwhelm.
Physical Signs
Dissociation can also affect how you experience your body.
You may notice:
Feeling disconnected from your body.
Feeling like your body doesn't belong to you.
Feeling numb or less aware of physical sensations.
Difficulty noticing hunger or thirst.
Difficulty recognizing pain until it becomes severe.
Feeling like you're moving on autopilot.
Feeling physically "checked out."
Feeling detached during physical touch.
Some survivors describe feeling as though they are floating or watching themselves from outside their body.
Cognitive Signs
Trauma can affect attention, concentration, and memory.
You may experience:
Difficulty concentrating.
Losing track of conversations.
Forgetting parts of your day.
Memory gaps.
Feeling mentally foggy.
Difficulty making decisions.
Losing track of time.
Feeling confused about what happened earlier in the day.
These symptoms can feel frightening, but they are common among people who experience trauma-related dissociation.
Feeling Unreal (Depersonalization)
Some survivors experience depersonalization, a type of dissociation in which they feel disconnected from themselves.
It may feel like:
You're watching yourself from outside your body.
Your body doesn't feel like your own.
You don't recognize yourself in the mirror.
Your movements don't feel fully under your control.
Your voice sounds unfamiliar.
You feel like you're living in someone else's body.
These experiences can be unsettling, but they are a recognized trauma response.
Feeling Like the World Isn't Real (Derealization)
Others experience derealization, in which the world around them feels strange or unreal.
You might notice:
Feeling like you're living in a dream.
Feeling as though the world looks foggy or distant.
Colors appearing muted.
Sounds feeling far away.
People seeming unfamiliar.
Your surroundings feeling unreal or artificial.
Feeling disconnected from time.
Even though these sensations feel strange, they do not mean you are losing touch with reality.
Most people experiencing derealization recognize that something feels "off," even though they know the world hasn't actually changed.
Losing Time
One of the more confusing signs of dissociation is losing track of time.
You may notice:
Not remembering parts of conversations.
Forgetting how you arrived somewhere.
Missing parts of a meeting or class.
Realizing hours have passed without remembering what happened.
Having gaps in your memory after stressful situations.
These experiences occur because your brain was focused on survival rather than forming detailed memories.
Dissociation During Stress
Many survivors notice that dissociation becomes more likely during situations that feel emotionally overwhelming.
For example:
During conflict.
During sexual intimacy.
During medical appointments.
When receiving criticism.
When feeling trapped.
During panic or anxiety.
After hearing about someone else's trauma.
When experiencing strong emotions.
Recognizing these patterns can help you better understand your nervous system.
Signs During Intimacy
Dissociation is especially common during sexual activity after sexual trauma.
You may notice:
Feeling emotionally absent during sex.
Difficulty staying present.
Feeling like you're going through the motions.
Losing awareness of physical sensations.
Feeling disconnected from pleasure.
Difficulty remembering parts of the experience afterward.
Feeling like your mind "leaves" during intimacy.
This is not a lack of love or attraction.
It is your nervous system trying to protect you.
Other Everyday Signs
Some signs of dissociation are easy to overlook.
You may notice that you:
Zone out frequently.
Stare into space without realizing it.
Feel like you're functioning on autopilot.
Have difficulty identifying your emotions.
Avoid thinking about certain memories.
Feel disconnected from your surroundings.
Struggle to stay focused during conversations.
Feel exhausted after emotionally stressful situations.
These experiences are often subtle but can have a significant impact on daily life.
Recognizing Dissociation Is Progress
Many survivors feel discouraged when they realize how often they dissociate.
In reality, recognizing dissociation is a sign of growth.
You cannot change what you don't notice.
The more aware you become of your nervous system's patterns, the more opportunities you have to respond with grounding, self-compassion, and support.
Awareness is one of the first steps toward healing.

Grounding Techniques
When someone experiences dissociation or becomes triggered, it can feel as though their mind has been pulled back into the past.
Grounding techniques are simple strategies that help bring your attention back to the present moment.
Grounding doesn't erase the trauma or stop difficult emotions immediately.
Instead, it helps remind your brain and nervous system that the trauma is over and you are safe right now.
Think of grounding as gently reconnecting your mind and body with the present.
The more you practice these skills, the easier they often become to use during stressful moments.
What Is Grounding?
Grounding is the practice of using your senses, body, or thoughts to reconnect with the present moment.
Grounding helps calm the nervous system by sending your brain a simple message:
"I'm here. I'm safe. The danger has passed."
Grounding is not about pretending everything is okay.
It is about helping your brain recognize the difference between the past and the present.
The 5-4-3-2-1 Technique
One of the most effective grounding exercises uses your five senses.
Slowly identify:
5 things you can see.
4 things you can touch.
3 things you can hear.
2 things you can smell.
1 thing you can taste.
Take your time.
There is no need to rush.
This exercise helps shift your attention away from traumatic memories and back to your current surroundings.
Feel Your Feet on the Ground
One of the simplest grounding techniques is noticing the support beneath you.
Try:
Pressing both feet firmly into the floor.
Feeling your shoes against your feet.
Noticing the texture of the ground.
Gently shifting your weight from one foot to the other.
Remind yourself:
"I am here."
"I am supported."
Slow Your Breathing
Trauma often causes breathing to become fast and shallow.
Slowing your breathing helps calm your nervous system.
Try this simple exercise:
Inhale slowly through your nose for 4 seconds.
Hold your breath for 2 seconds.
Exhale gently through your mouth for 6 seconds.
Repeat several times.
A longer exhale tells your brain that it can begin to relax.
Orient Yourself to Your Environment
One of the fastest ways to help your nervous system recognize safety is to slowly look around your environment.
Notice:
The colors in the room.
The furniture around you.
The windows.
The lighting.
The people who are present.
Then ask yourself:
Where am I?
What is today's date?
How old am I?
Who is with me?
Am I safe right now?
These questions help your thinking brain reconnect with the present.
Hold a Comforting Object
Some people find it helpful to carry a grounding object.
Examples include:
A smooth stone.
A favorite piece of jewelry.
A stress ball.
A small stuffed animal.
A meaningful keychain.
A piece of fabric with an interesting texture.
Focus on how the object feels in your hand.
Notice:
Its temperature.
Its weight.
Its texture.
Its shape.
This simple exercise helps anchor you in the present.
Use Temperature
Temperature changes can quickly bring your attention back to your body.
You might try:
Holding an ice cube.
Splashing cool water on your face.
Washing your hands with warm water.
Holding a warm mug of tea.
Wrapping yourself in a soft blanket.
Notice the sensations without judging them.
Move Your Body
Movement helps release survival energy that may still be stored in your nervous system.
Try:
Stretching.
Walking.
Shaking out your hands and arms.
Rolling your shoulders.
Gentle yoga.
Dancing.
Progressive muscle relaxation.
Even a few minutes of movement can help you reconnect with your body.
Name What Is Happening
Sometimes simply naming your experience can reduce its intensity.
You might say:
"I'm feeling triggered."
"I'm beginning to dissociate."
"This is a trauma response."
"My nervous system is trying to protect me."
Naming what is happening helps activate the logical part of your brain.
Use Reassuring Statements
Gentle reminders can help calm the nervous system.
You might repeat:
"I am safe."
"The trauma is over."
"This is a memory, not my current reality."
"I survived."
"My body is trying to protect me."
"This feeling will pass."
"I don't have to face this alone."
Choose statements that feel believable and comforting to you.
Connect With Someone Safe
Sometimes the most powerful grounding tool is another person.
If possible, reach out to someone you trust.
You might:
Call a friend.
Text a loved one.
Sit quietly with your partner.
Talk with your therapist.
Ask someone to simply stay with you.
Safe relationships help teach the nervous system that connection is possible again.
Create a Grounding Kit
Many survivors find it helpful to keep a small grounding kit nearby.
Your kit might include:
A calming scent, such as lavender.
Gum or mints.
A comforting object.
Headphones with calming music.
A list of grounding reminders.
Family photos.
A journal.
Positive affirmation cards.
Having these tools ready can make grounding easier during difficult moments.
Practice Before You Need It
Grounding works best when it becomes familiar.
Rather than waiting until you're overwhelmed, practice these skills during calm moments.
The more often you practice, the more naturally your brain will remember them when you're triggered.
Like any skill, grounding becomes easier with repetition.
Grounding Is Not About Perfection
Some days, grounding works quickly.
Other days, it may take longer.
That doesn't mean you're doing it wrong.
Healing isn't about making distress disappear instantly.
It's about helping your nervous system slowly return to a place of safety.
Every time you practice grounding, you're teaching your brain something new:
The danger is over.
I can come back to the present.

Reconnecting With Your Body
One of the most painful effects of sexual trauma is feeling disconnected from your own body.
Many survivors describe feeling like their body no longer belongs to them. Others avoid looking at themselves in the mirror, dislike being touched, or feel numb to physical sensations. Some say they feel as though they are living "from the neck up," disconnected from the body that carried them through the trauma.
If this sounds familiar, you are not alone.
Trauma can change the way we experience our bodies.
The encouraging news is that this disconnection does not have to be permanent.
Healing often involves slowly rebuilding a relationship with your body—one that is based on safety, trust, compassion, and choice.
Why Trauma Causes Disconnection
During a traumatic experience, disconnecting from the body can be an incredibly effective survival strategy.
If the body feels overwhelmed by fear, pain, or helplessness, the brain may reduce awareness of physical sensations through dissociation.
This response helps people survive experiences that feel unbearable.
The challenge is that the nervous system may continue using this strategy long after the trauma has ended.
Instead of feeling connected to your body, you may feel distant from it.
Your body isn't rejecting you.
It learned that disconnecting helped you survive.
Your Body Is Not the Enemy
Many survivors feel angry with their bodies.
They may think:
"My body betrayed me."
"I hate my body."
"I don't trust my body anymore."
"I don't feel safe in my own skin."
"I wish I could escape my body."
These thoughts are understandable.
But your body did not betray you.
Your body did everything it could to help you survive.
Every survival response—freezing, dissociating, becoming numb, or complying—was your nervous system trying to keep you alive.
Your body deserves compassion, not blame.
Signs You May Feel Disconnected From Your Body
You might notice:
Feeling emotionally numb.
Feeling physically numb.
Avoiding mirrors.
Avoiding physical touch.
Difficulty recognizing hunger or fullness.
Difficulty noticing pain.
Feeling uncomfortable in your own skin.
Feeling detached during intimacy.
Feeling like your body doesn't belong to you.
Difficulty identifying emotions because they often begin as body sensations.
These experiences are common after sexual trauma.
Reconnection Happens Slowly
Many survivors believe they should immediately feel comfortable in their bodies again.
Healing rarely works that way.
Rebuilding trust with your body is much like rebuilding trust with another person.
It happens through many small, safe experiences over time.
There is no need to rush.
Every small moment of safety matters.
Start With Neutral Awareness
You do not have to love your body to begin reconnecting with it.
Sometimes the first step is simply noticing it without judgment.
For example:
Notice your feet touching the floor.
Notice your breathing.
Notice your hands resting in your lap.
Feel the chair supporting your body.
Notice warmth or coolness on your skin.
The goal is awareness—not evaluation.
Gentle Movement
Movement can help rebuild a sense of connection with your body.
Choose activities that feel safe and enjoyable.
Examples include:
Walking.
Stretching.
Yoga.
Swimming.
Dancing.
Gardening.
Gentle strength training.
Hiking.
Focus less on exercise and more on noticing how your body feels while moving.
Ask yourself:
"What does my body need today?"
Practice Mindful Touch
Trauma can make physical touch feel complicated.
One way to rebuild safety is through gentle, self-directed touch.
Examples include:
Wrapping yourself in a soft blanket.
Holding your own hands.
Applying lotion slowly.
Taking a warm bath.
Brushing your hair mindfully.
Placing a hand over your heart while breathing.
The goal is to remind your nervous system that touch can also be comforting and safe.
Listen to Your Body
Healing often involves learning to notice your body's signals again.
Ask yourself throughout the day:
Am I hungry?
Am I thirsty?
Am I tired?
Am I cold?
Am I tense?
Do I need a break?
Responding to these needs teaches your nervous system that your body deserves care.
Reclaim Choice
Trauma often takes away choice.
Healing gives it back.
Practice making small choices about your body.
For example:
Choosing what clothes feel comfortable.
Saying yes when you want touch.
Saying no when you don't.
Choosing when to rest.
Choosing how you move.
Choosing who has access to your body.
Every healthy choice reinforces an important message:
My body belongs to me.
Explore Safe Pleasure
Reconnecting with your body isn't only about reducing distress.
It's also about rediscovering comfort, joy, and pleasure.
Pleasure doesn't have to be sexual.
It might include:
Feeling sunshine on your face.
Taking a warm shower.
Drinking your favorite tea or coffee.
Petting an animal.
Listening to music.
Laughing with a friend.
Stretching after waking up.
Sitting outside in nature.
These small experiences help teach your nervous system that your body can experience safety and enjoyment again.
Practice Self-Compassion
Many survivors speak to themselves in ways they would never speak to someone they love.
Notice your inner dialogue.
Instead of saying:
"My body is broken."
Try saying:
"My body has been protecting me."
Instead of:
"I hate my body."
Try:
"My body survived something incredibly difficult."
The words you use matter.
Compassion creates safety.
Safety creates healing.
Trauma-Informed Therapies Can Help
You do not have to reconnect with your body alone.
Many evidence-based treatments help survivors rebuild a sense of safety and connection.
These include:
Somatic therapies.
Sensorimotor Psychotherapy.
Internal Family Systems (IFS).
Mindfulness-based therapies.
Trauma-informed yoga.
Pelvic floor physical therapy.
These approaches work by helping both the brain and body process traumatic experiences and develop new patterns of safety.
Your Body Is Still Yours
Trauma may have changed your relationship with your body.
It did not take away your right to feel safe inside it.
Your body has carried you through every difficult moment of your life.
It has protected you in remarkable ways.
Now, healing is about helping your body experience something new.
Safety.
Choice.
Comfort.
Connection.
You do not have to force yourself to love your body overnight.
Simply becoming curious about it is enough.
One breath.
One moment.
One small act of kindness toward yourself at a time.
Part 7: Healing Is Possible
What Recovery Really Looks Like
If you've experienced sexual trauma, you may wonder whether healing is actually possible.
You may have asked yourself:
"Will I ever feel normal again?"
"Will I always be triggered?"
"Will I ever trust anyone again?"
"Will sex ever feel safe?"
"Will I always feel broken?"
These are some of the most common questions survivors ask.
The answer is one I wish every survivor could hear:
Healing is absolutely possible.
Not because the trauma disappears.
Not because you'll forget what happened.
But because your brain, body, and nervous system have an incredible ability to heal.
Recovery is not about becoming the person you were before the trauma.
It is about becoming someone who no longer has to live in survival mode.
Healing Is Not Forgetting
One of the biggest misconceptions about trauma recovery is that healing means forgetting.
It doesn't.
Most survivors will always remember what happened.
The difference is that the memory changes.
Instead of feeling like the trauma is happening all over again, it begins to feel like something that happened in the past.
You remember it.
You don't relive it.
That is one of the biggest goals of trauma therapy.
Healing Doesn't Mean the Trauma Never Happened
Recovery doesn't erase your story.
It doesn't excuse the person who harmed you.
It doesn't pretend everything is okay.
Healing simply means that what happened no longer controls every part of your life.
You may still remember.
You may still grieve.
But the trauma no longer gets to make every decision for you.
Healing Is Not Linear
Many survivors expect recovery to happen in a straight line.
They imagine that once they start feeling better, they'll continue improving every day.
Real healing doesn't usually work that way.
Recovery often looks like:
Two steps forward and one step back.
Good days and difficult days.
Progress followed by setbacks.
Feeling hopeful one week and discouraged the next.
This is completely normal.
A difficult day does not erase your progress.
Healing is measured over months and years—not moments.
Healing Often Happens Quietly
Many survivors expect healing to feel dramatic.
More often, it happens in small moments.
One day you notice:
You slept through the night.
A trigger didn't feel quite as intense.
You laughed without forcing it.
You enjoyed being hugged.
You stood up for yourself.
You asked for what you needed.
You looked in the mirror with less criticism.
You felt present during intimacy.
You realized you hadn't thought about the trauma all day.
These moments may seem small.
They are actually signs that your nervous system is changing.
Recovery Is About Safety
Trauma teaches the brain that the world is dangerous.
Healing teaches the brain that safety is possible again.
That safety begins with:
Yourself.
Your body.
Safe relationships.
Healthy boundaries.
Self-compassion.
Consistency.
The nervous system heals through repeated experiences of safety.
Not through forcing yourself to "get over it."
Healing Doesn't Mean You Won't Get Triggered
Many survivors worry that getting triggered means they aren't healing.
Triggers may still happen.
The difference is often how you respond.
As healing progresses, many people notice:
Triggers happen less often.
Triggers feel less intense.
Recovery happens more quickly.
They have tools to calm themselves.
They trust themselves more.
Healing isn't measured by never being triggered.
It's measured by how much power the triggers have over your life.
Relationships Can Heal Too
Sexual trauma often affects trust and intimacy.
Many survivors wonder if they'll ever be able to have a healthy relationship.
The answer is yes.
Healthy relationships don't require perfect healing.
They require:
Honesty.
Communication.
Patience.
Respect.
Consent.
Emotional safety.
Many survivors discover that safe relationships become part of the healing process.
Your Brain Can Change
One of the most hopeful discoveries in neuroscience is that the brain remains capable of change throughout life.
This is called neuroplasticity.
Your brain learned survival patterns because they helped protect you.
It can also learn new patterns based on safety.
With repeated experiences of safety and evidence-based treatment, the brain can become less reactive, the nervous system can become more regulated, and traumatic memories can become less distressing.
Healing is not wishful thinking.
It is something the brain is biologically capable of doing.
You Don't Have to Heal Alone
Recovery is not something you have to figure out by yourself.
Many survivors benefit from working with trauma-informed professionals, including:
Trauma therapists.
Pelvic floor physical therapists.
Psychiatrists when appropriate.
Support groups.
Trusted medical providers.
Healing often happens in safe relationships.
You deserve people who help you feel seen, believed, and supported.
There Is No "Right" Way to Heal
Every survivor's journey is different.
Some people heal through therapy.
Others find healing through supportive relationships, spirituality, movement, creativity, advocacy, or community.
Most people use a combination of many different approaches.
There is no timeline.
There is no perfect path.
The only goal is finding what helps you feel safer, more connected, and more like yourself.
You Are More Than What Happened to You
Trauma may always be part of your story.
It is not your entire story.
You are more than your symptoms.
More than your triggers.
More than your diagnosis.
More than what someone else chose to do.
You are still capable of:
Love.
Trust.
Joy.
Intimacy.
Connection.
Pleasure.
Confidence.
Hope.
None of those things were destroyed.
They may have been buried beneath survival.
Healing is about uncovering them again.
What Recovery Really Looks Like
Recovery isn't becoming fearless.
It's learning that fear doesn't have to make your decisions.
Recovery isn't never thinking about the trauma.
It's remembering without reliving.
Recovery isn't pretending the pain never existed.
It's realizing the pain no longer controls your future.
Recovery looks like:
Setting boundaries without guilt.
Feeling safe in your own body.
Trusting yourself again.
Feeling present during intimacy.
Sleeping more peacefully.
Experiencing joy without apology.
Loving without constant fear.
Choosing relationships that honor your worth.
Believing you deserve healing.
Recovery isn't perfection.
Recovery is freedom.
Healing Is Possible
There may have been a time when surviving was your greatest accomplishment.
Now, your goal doesn't have to be survival.
It can be living.
Healing is not about becoming who you were before the trauma.
It is about becoming who you were always meant to be—someone whose life is no longer defined by what happened to them.
Your story did not end with the trauma.
In many ways, this is where a new chapter begins.
Neuroplasticity and Healing
One of the most hopeful discoveries in modern neuroscience is that the brain can change throughout your entire life.
This ability is called neuroplasticity.
For many years, scientists believed that the adult brain was relatively fixed and unable to change. We now know that isn't true.
Every experience you have—every thought, memory, relationship, and skill—changes your brain.
That means the same brain that adapted to survive trauma can also adapt to heal from it.
This is one of the reasons recovery from sexual trauma is possible.
What Is Neuroplasticity?
Neuroplasticity is the brain's ability to form new neural connections, strengthen healthy pathways, and weaken pathways that are no longer needed.
Think of your brain like a network of hiking trails.
The more often you walk down one trail, the wider and easier it becomes.
Trauma repeatedly activates the brain's "danger" pathways.
The nervous system becomes incredibly efficient at detecting threats because those pathways have been used over and over again.
Healing works in the opposite direction.
As you repeatedly experience safety, connection, and regulation, your brain begins building new pathways that support calm, trust, and resilience.
How Trauma Changes the Brain
Trauma changes the brain because the brain is trying to help you survive.
After sexual trauma, many survivors experience changes in several brain regions.
The amygdala, the brain's alarm system, often becomes more sensitive and reacts more quickly to potential danger.
The prefrontal cortex, which helps with logical thinking and emotional regulation, may become less active during times of stress.
The hippocampus, which helps organize memories and distinguish the past from the present, may have difficulty placing traumatic memories into a clear timeline.
These changes are adaptations.
Your brain reorganized itself to increase your chances of surviving.
The Brain Can Learn Safety Again
The remarkable part is that these changes are not necessarily permanent.
Just as the brain learned danger, it can also learn safety.
Each time you experience:
A safe relationship.
A healthy boundary.
A calm conversation.
A successful grounding exercise.
A positive therapy session.
A peaceful moment in nature.
A supportive touch that you choose.
your brain receives new information.
Instead of learning:
"The world is dangerous."
it slowly begins learning:
"Safety is possible."
These repeated experiences strengthen new neural pathways.
Small Changes Matter
Many survivors become discouraged because healing feels slow.
But neuroplasticity happens through repetition, not dramatic breakthroughs.
Every time you:
Practice grounding.
Challenge a negative belief.
Set a healthy boundary.
Calm your nervous system.
Stay present during a trigger.
Ask for help.
Show yourself compassion.
you are literally helping reshape your brain.
These small moments may not feel significant.
Biologically, they are.
Why Therapy Works
Evidence-based trauma treatments work because they take advantage of neuroplasticity.
Therapies such as:
Somatic therapies.
Mindfulness-based interventions.
help the brain process traumatic memories differently.
Rather than repeatedly activating survival pathways, these therapies help the brain create new, healthier connections.
Over time, traumatic memories become less emotionally overwhelming because the brain has updated how it stores and responds to them.
Your Nervous System Learns Through Experience
Healing doesn't happen because you tell yourself to "get over it."
Your nervous system learns through lived experiences.
For example:
The first time you set a boundary, your body may panic.
The tenth time, it may feel uncomfortable.
The hundredth time, it may feel natural.
That's neuroplasticity.
The same process happens with trust, intimacy, emotional regulation, and self-compassion.
The more often your nervous system experiences safety, the more familiar safety becomes.
Healing Is Like Building a Muscle
Imagine going to the gym for the first time.
One workout won't dramatically change your body.
But consistent practice over weeks and months creates lasting change.
Healing works the same way.
Each healthy choice strengthens new neural pathways.
Eventually, those healthier pathways become stronger than the old survival patterns.
Progress often happens so gradually that you don't notice it until you look back.
Neuroplasticity Gives Hope
One of the most damaging beliefs trauma creates is:
"I'll always be this way."
Neuroplasticity tells us otherwise.
Your brain is not permanently damaged.
It has been shaped by your experiences.
And experiences can continue shaping it throughout your life.
This doesn't mean healing is easy.
It doesn't mean trauma disappears.
It means your future is not determined by your past.
Your Brain Wants to Heal
Just as your body naturally begins healing after a cut or broken bone, your brain is constantly trying to heal itself.
Sleep strengthens new memories.
Positive relationships regulate the nervous system.
Movement supports brain health.
Learning creates new neural connections.
Therapy helps reorganize traumatic memories.
Healing is not something you force.
It is something you support.
Healing Is Happening Even When You Don't Feel It
Many survivors become discouraged because they don't feel dramatically different after a few therapy sessions.
The brain doesn't usually heal overnight.
It changes through thousands of small moments of safety.
One day you notice you're less reactive.
Another day you recover from a trigger more quickly.
Weeks later you realize you slept through the night.
Months later you notice intimacy feels safer.
Those changes are signs that your brain has been quietly rewiring itself all along.

Building Safety Again
Healing from sexual trauma begins with one essential ingredient: safety.
Trauma teaches the brain and nervous system that the world is dangerous. It teaches your body to stay alert, your mind to expect harm, and your nervous system to prepare for danger—even when you are no longer in a threatening situation.
Healing teaches something entirely different.
It teaches your brain that the danger is over.
It teaches your body that it can finally rest.
It teaches your nervous system that safety is possible again.
Building safety is not something that happens overnight. It develops through hundreds of small experiences that slowly convince your brain that life is different now than it was during the trauma.
Why Safety Comes First
When your nervous system believes you are in danger, survival becomes its only priority.
That makes it difficult to:
Relax.
Trust other people.
Sleep peacefully.
Experience pleasure.
Feel emotionally connected.
Concentrate.
Be fully present.
Enjoy intimacy.
This isn't because something is wrong with you.
It's because your brain is doing exactly what it was designed to do—protect you.
Before your brain can fully process trauma, it first needs repeated experiences of feeling safe.
Safety Is a Feeling, Not Just a Place
Many people assume safety simply means being somewhere dangerous things aren't happening.
For trauma survivors, safety is much more than that.
Safety is something your nervous system experiences.
You can be sitting in a perfectly safe room and still feel terrified.
You can also be in a busy environment and feel calm because your nervous system recognizes that you are no longer in danger.
Healing focuses on helping your body experience safety—not just understand it intellectually.
Safety Looks Different for Everyone
There is no universal definition of safety.
Every survivor has different experiences, different triggers, and different needs.
You might feel safest when you:
Spend time in nature.
Lock your front door.
Sit under a weighted blanket.
Listen to calming music.
Have predictable routines.
Know where the exits are.
Spend time with trusted people.
Have quiet time alone.
The goal is not to make your safety look like someone else's.
The goal is to discover what helps your own nervous system relax.
Rebuilding Safety in Your Body
Sexual trauma often changes the relationship you have with your body.
Many survivors no longer feel at home in their own skin.
Some avoid physical sensations.
Others feel disconnected from their bodies altogether.
Healing begins by helping your body experience comfort again.
This may include:
Practicing slow, intentional breathing.
Using grounding techniques.
Going for gentle walks.
Stretching or practicing yoga.
Getting enough sleep.
Eating nourishing meals.
Drinking enough water.
Spending time outside.
Noticing pleasant physical sensations.
These simple experiences teach your nervous system that your body can be a place of comfort instead of danger.
Rebuilding Emotional Safety
Trauma can make emotions feel overwhelming or unsafe.
Some survivors learned to hide their feelings.
Others learned to disconnect from them completely.
Healing involves slowly creating enough safety to experience emotions without becoming overwhelmed.
You might begin by:
Naming your emotions.
Journaling.
Talking with someone you trust.
Practicing mindfulness.
Allowing yourself to cry.
Celebrating moments of joy.
Speaking to yourself with kindness.
The goal isn't to eliminate difficult emotions.
It's to learn that emotions can be experienced safely.
Rebuilding Safety in Relationships
Sexual trauma often affects the ability to trust others.
You may find yourself expecting rejection, betrayal, or harm, even from people who have earned your trust.
This is your nervous system trying to protect you.
Healthy relationships help rewrite those expectations.
Safe relationships are built on:
Respect.
Honesty.
Consent.
Reliability.
Healthy communication.
Emotional support.
Mutual trust.
Consistent boundaries.
Every healthy relationship gives your brain another opportunity to learn that not everyone is unsafe.
Reclaiming Your Right to Choose
One of the deepest wounds of sexual trauma is the loss of choice.
Someone else took away your ability to decide what happened to your body.
Healing involves reclaiming that choice.
This can happen in everyday moments.
You might choose:
To say no without apologizing.
To ask for what you need.
To leave situations that feel uncomfortable.
To change your mind.
To slow down.
To take breaks.
To decide who has access to your body.
Every healthy decision sends your nervous system an important message:
"My body belongs to me."
Creating Predictability
Trauma is often chaotic and unpredictable.
Predictable routines help calm the nervous system because they reduce uncertainty.
Simple routines can make a surprising difference.
Examples include:
Waking up at the same time each morning.
Going to bed on a consistent schedule.
Eating regular meals.
Taking daily walks.
Practicing grounding exercises.
Creating a calming bedtime routine.
These small habits help your brain recognize that life is becoming more stable.
Safety Before Processing
Many survivors want to immediately work through the trauma itself.
While processing traumatic memories is an important part of recovery, it is usually not the first step.
Trauma-informed therapy often follows this sequence:
Build safety and emotional regulation.
Process traumatic memories.
Strengthen connection and move forward.
Without a foundation of safety, processing trauma can feel overwhelming.
Safety prepares your nervous system for healing.
Learning to Trust Yourself Again
Trauma often damages self-trust.
You may question your instincts, your memories, or your decisions.
Healing involves rebuilding confidence in yourself.
You begin learning that:
You can recognize safe people.
You can set healthy boundaries.
You can protect yourself.
You can listen to your body's signals.
You can make decisions that honor your needs.
Trust grows one experience at a time.
Self-Compassion Creates Safety
One of the most healing things you can do is change the way you speak to yourself.
Instead of saying:
"I should be over this."
Try saying:
"I'm healing from something incredibly difficult."
Instead of asking:
"What's wrong with me?"
Try asking:
"What does my nervous system need right now?"
Compassion helps calm the brain.
Shame keeps the nervous system stuck in survival mode.
The more kindness you offer yourself, the safer your inner world becomes.
Safety Is Built Through Repetition
Healing doesn't happen because of one breakthrough.
It happens because your brain repeatedly experiences safety.
Every time you:
Practice grounding.
Calm your breathing.
Set a healthy boundary.
Spend time with someone you trust.
Care for your body.
Honor your limits.
Speak kindly to yourself.
you are strengthening new neural pathways.
Little by little, your brain begins believing a new story:
"I am safe now."
Healing Expands Your World
As your sense of safety grows, so does your life.
You may notice yourself trying things that once felt impossible.
Maybe you enjoy being hugged again.
Maybe you travel without constant anxiety.
Maybe you trust a partner.
Maybe intimacy begins to feel comforting instead of frightening.
These moments are signs that your nervous system is healing.
Safety creates freedom.
You Deserve to Feel Safe
You do not have to earn safety.
You do not have to prove that you deserve peace.
You deserve relationships where your boundaries are respected.
You deserve a body that feels like home.
You deserve to rest without constantly scanning for danger.
You deserve love that feels safe.
You deserve joy without fear.
Most importantly, you deserve to believe that healing is possible.
What Progress Can Look Like
One of the biggest misconceptions about healing from sexual trauma is that progress should be obvious.
Many survivors expect recovery to feel dramatic.
They imagine waking up one day and suddenly feeling completely different.
In reality, healing usually happens much more quietly.
It often shows up in small moments that are easy to overlook.
You may not notice how much you've changed until you look back and realize how far you've come.
Progress is rarely about never struggling again.
It's about struggling differently.
It's about recovering more quickly, feeling safer more often, and spending less time living in survival mode.
Progress Doesn't Mean You're Never Triggered
Many survivors believe they have failed if they still experience triggers.
This simply isn't true.
Healing doesn't mean triggers disappear overnight.
Instead, you may notice:
Triggers happen less often.
Triggers feel less overwhelming.
You recognize them more quickly.
You recover faster.
You know what helps calm your nervous system.
You trust yourself to get through them.
Recovery is not measured by the absence of triggers.
It is measured by your growing ability to respond to them with confidence and compassion.
Progress Can Be Small
Some of the biggest signs of healing are surprisingly ordinary.
Progress might look like:
Sleeping through the night.
Going an entire day without thinking about the trauma.
Looking at yourself in the mirror with kindness.
Taking a deep breath instead of panicking.
Asking for help.
Saying no without feeling guilty.
Feeling your emotions instead of shutting down.
Laughing without forcing it.
Feeling comfortable in silence.
Looking forward to the future.
These moments may seem small.
They are actually evidence that your nervous system is changing.
Progress in Your Body
As healing continues, many survivors notice changes in how their body responds.
You may notice:
Less muscle tension.
Better sleep.
Fewer headaches.
Feeling more connected to your body.
Less hypervigilance.
Feeling calmer in situations that once felt overwhelming.
Enjoying physical affection again.
Feeling more comfortable with your own body.
Your body begins learning that it no longer has to stay on high alert.
Progress in Your Relationships
Healing often becomes visible in the way you relate to other people.
You might notice that you:
Trust people more easily.
Set healthier boundaries.
Communicate your needs.
Feel safer asking for support.
Allow yourself to be vulnerable.
Choose healthier relationships.
Recognize red flags sooner.
Feel more connected during conversations.
Believe that healthy love is possible.
You may also find yourself walking away from relationships that no longer feel safe.
That is progress, too.
Progress in Your Sexuality
Healing after sexual trauma often changes your relationship with intimacy.
You may notice:
Feeling less anxious before intimacy.
Feeling more present during sex.
Enjoying physical touch.
Feeling more comfortable saying yes or no.
Experiencing increased desire.
Feeling less shame.
Becoming more connected to pleasure.
Feeling emotionally closer to your partner.
Healing is not measured by how often you have sex.
It is measured by how safe, connected, and authentic you feel when you choose intimacy.
Progress in Your Thoughts
Trauma often changes the way people think about themselves.
As healing occurs, you may notice thoughts beginning to shift.
Instead of thinking:
"I'm broken."
You begin thinking:
"I'm healing."
Instead of:
"It was my fault."
You begin believing:
"I survived something that never should have happened."
Instead of:
"I'll never trust anyone."
You begin wondering:
"Maybe safe people do exist."
Changing these beliefs takes time.
Each new thought represents another step toward recovery.
Progress Doesn't Erase Hard Days
Healing does not mean every day feels easy.
Even years into recovery, there may still be moments that feel difficult.
You may still:
Feel triggered.
Become emotional.
Experience grief.
Feel overwhelmed during stressful periods.
Having difficult days does not erase your healing.
Think about recovering from a physical injury.
Even after a broken bone heals, it may ache during cold weather.
That doesn't mean it never healed.
Trauma recovery works much the same way.
Progress Is Learning to Trust Yourself
One of the greatest signs of healing is rebuilding trust in yourself.
You begin believing:
I can recognize danger.
I can protect myself.
I can set boundaries.
I can ask for help.
I can make healthy decisions.
I can listen to my body.
I can handle difficult emotions.
That confidence often becomes one of the most meaningful parts of recovery.
Progress Is Living More Than Surviving
Perhaps the biggest sign of healing is that your life slowly becomes bigger than your trauma.
You begin thinking less about surviving and more about living.
You make plans.
You dream about the future.
You laugh more.
You feel curious again.
You discover hobbies.
You deepen friendships.
You experience love.
You allow yourself to hope.
Trauma may still be part of your story.
It is no longer the entire story.
Celebrate Every Victory
Many survivors overlook their progress because they focus only on what still feels difficult.
Take time to recognize your victories.
Celebrate when you:
Set a boundary.
Go to therapy.
Get out of bed on a hard day.
Practice grounding.
Ask for support.
Speak kindly to yourself.
Feel present during a trigger.
Take care of your body.
Allow yourself to rest.
Healing is built from these moments.
Every one of them matters.
There Is No Finish Line
Recovery is not about becoming a perfect version of yourself.
It is about building a life that feels increasingly safe, meaningful, and authentic.
Some days healing will feel obvious.
Other days it will feel invisible.
Trust that growth is still happening.
Your brain is changing.
Your nervous system is learning.
Your confidence is growing.
Little by little, your life becomes less organized around fear and more organized around freedom.
Part 8: Evidence-Based Treatments for Sexual Trauma
Eye Movement Desensitization and Reprocessing (EMDR) Therapy
One of the most effective treatments for sexual trauma is Eye Movement Desensitization and Reprocessing, commonly known as EMDR.
EMDR is an evidence-based psychotherapy that helps the brain process traumatic memories so they become less emotionally overwhelming.
Rather than simply teaching you how to cope with symptoms, EMDR helps address the underlying memories that continue to keep the nervous system stuck in survival mode.
Today, EMDR is recommended by many national and international organizations as an effective treatment for post-traumatic stress disorder (PTSD) and other trauma-related conditions.
For many survivors of sexual trauma, EMDR has been life-changing.
What Is EMDR?
Eye Movement Desensitization and Reprocessing (EMDR) is a structured psychotherapy that helps the brain reprocess traumatic memories.
Unlike traditional talk therapy, EMDR does not require you to describe every detail of your traumatic experience repeatedly.
Instead, your therapist helps you safely activate a traumatic memory while using a process called bilateral stimulation.
Bilateral stimulation typically involves:
Moving your eyes back and forth.
Alternating taps on your hands or knees.
Alternating sounds through headphones.
This process helps the brain reorganize how traumatic memories are stored.
Over time, the memories remain, but they no longer feel like they are happening in the present.
How Trauma Gets "Stuck"
Under normal circumstances, the brain naturally processes daily experiences.
Most memories gradually become part of your life story.
You can remember them without feeling overwhelmed.
Traumatic experiences are different.
When something is extremely frightening or overwhelming, the brain may not fully process the event.
Instead, the memory can become "stuck."
The images, emotions, body sensations, and beliefs connected to the trauma remain highly activated.
This is why survivors often feel as though the trauma is happening all over again when they are triggered.
EMDR helps the brain finish processing these memories.
How Does EMDR Work?
Researchers are still studying exactly how EMDR works, but we know that it helps the brain integrate traumatic memories more effectively.
During EMDR therapy, you briefly focus on a traumatic memory while engaging in bilateral stimulation.
As your brain processes the memory, new insights, emotions, thoughts, and connections often emerge naturally.
Over time, many survivors notice that:
The memory feels more distant.
The emotional intensity decreases.
Physical reactions become less severe.
Negative beliefs begin to change.
Triggers become less overwhelming.
They feel more present in daily life.
The goal is not to erase your memories.
The goal is to help your brain recognize that the trauma is over.
What Happens During an EMDR Session?
Many people worry that EMDR means reliving their trauma.
That is not the goal.
A typical EMDR treatment includes several stages.
First, you and your therapist work together to build coping skills and ensure you have enough emotional stability before processing traumatic memories.
Once you are ready, you'll identify a specific memory to work on.
Your therapist will ask you to notice:
An image connected to the memory.
The emotions you experience.
Physical sensations in your body.
Negative beliefs about yourself.
Positive beliefs you would rather believe.
While focusing on these experiences, you'll engage in bilateral stimulation.
Your therapist will periodically pause and ask what you're noticing.
The process continues until the memory becomes significantly less distressing.
What Conditions Can EMDR Treat?
Although EMDR is best known for treating PTSD, research has shown it can help with many trauma-related concerns, including:
Sexual assault.
Childhood sexual abuse.
Military sexual trauma.
Human trafficking.
Intimate partner violence.
Medical trauma.
Anxiety.
Panic attacks.
Phobias.
Grief.
Depression.
Performance anxiety.
Negative self-beliefs.
Many survivors of sexual trauma also notice improvements in self-esteem, emotional regulation, relationships, and intimacy after treatment.
What Does the Research Say?
EMDR is one of the most extensively researched trauma therapies available.
Numerous clinical studies have found that EMDR is effective in reducing symptoms of PTSD, anxiety, depression, and trauma-related distress.
Many people experience meaningful improvement in fewer sessions than traditional trauma-focused talk therapy, although the exact length of treatment varies depending on the individual and the complexity of the trauma.
Organizations including the American Psychological Association (APA), the International Society for Traumatic Stress Studies (ISTSS), the Department of Veterans Affairs (VA), the Department of Defense (DoD), and the World Health Organization (WHO) recognize EMDR as an effective treatment for trauma.
Will I Forget What Happened?
No.
EMDR does not erase memories.
You will still know what happened.
The difference is that the memories often become less emotionally and physically overwhelming.
Many survivors describe it this way:
"I remember it, but I don't feel like I'm reliving it anymore."
That is one of the primary goals of trauma treatment.
Does EMDR Mean I Have to Talk About Everything?
Not necessarily.
Although your therapist needs enough information to guide treatment safely, EMDR does not require you to describe every detail of the traumatic experience.
Many survivors appreciate that they do not have to repeatedly tell their entire story.
The focus is on helping your brain heal—not forcing you to relive painful memories.
Is EMDR Right for Everyone?
EMDR is highly effective for many people, but every survivor is different.
Some individuals benefit from additional preparation before beginning trauma processing.
Others may combine EMDR with:
Traditional talk therapy.
Somatic therapies.
Medication.
Mindfulness practices.
A trained trauma therapist can help determine the best treatment plan based on your individual needs and goals.
Healing Is More Than Processing Trauma
One of the greatest strengths of EMDR is that it doesn't simply reduce symptoms.
It also helps people reconnect with themselves.
As traumatic memories become less overwhelming, many survivors notice that they:
Feel calmer.
Sleep better.
Trust themselves more.
Feel safer in relationships.
Experience fewer triggers.
Feel more connected to their bodies.
Enjoy greater emotional freedom.
Experience intimacy with less fear.
Healing often extends far beyond the traumatic memories themselves.

Somatic Therapy
Somatic therapy is a trauma treatment that focuses on the connection between the mind and body.
Because trauma is stored not only in our memories but also in our nervous system, many survivors continue to experience symptoms such as muscle tension, hypervigilance, chronic pain, dissociation, or feeling disconnected from their bodies long after the traumatic event has ended.
Somatic therapy helps people become more aware of their body's signals and teaches the nervous system how to move from survival mode back into a state of safety.
Treatment may include:
Mindful awareness of body sensations.
Breathing exercises.
Grounding techniques.
Gentle movement.
Learning to notice and regulate nervous system responses.
Unlike traditional talk therapy, the focus is less on telling the story of what happened and more on noticing how trauma is experienced in the body and helping the body release patterns of chronic stress and protection.
Somatic therapy is often used alongside treatments such as EMDR or traditional psychotherapy. Many survivors find that combining approaches helps them reconnect with their bodies, reduce physical symptoms of trauma, and experience a greater sense of safety.
Internal Family Systems (IFS)
Internal Family Systems (IFS) is a trauma-informed therapy that helps people understand the different "parts" of themselves that developed to cope with difficult experiences.
For example, after sexual trauma, you may have one part that avoids intimacy to stay safe, another part that feels shame, and another part that desperately wants connection. Rather than seeing these parts as problems, IFS views them as protective responses that developed to help you survive.
The goal of IFS is to help you understand these different parts with curiosity and compassion, while strengthening your core sense of self—the calm, confident, and compassionate part of you that can lead your healing.
IFS can help survivors:
Reduce shame and self-criticism.
Better understand their emotional reactions.
Heal inner conflict.
Increase self-compassion.
Feel more connected to themselves and others.
IFS is often used alongside other evidence-based trauma treatments, such as EMDR, to help survivors process traumatic experiences while building greater emotional understanding and self-acceptance.
Sex Therapy
For many survivors, healing from sexual trauma doesn't end when the traumatic memories become less distressing.
Even after significant healing, many people continue to struggle with intimacy, desire, arousal, orgasm, pain during sex, erectile dysfunction, body image concerns, shame, or feeling emotionally disconnected during sexual experiences.
This is where sex therapy can play an important role.
Sex therapy is a specialized form of psychotherapy that helps individuals and couples address the emotional, psychological, relational, and sexual effects of trauma in a safe, supportive, and nonjudgmental environment.
One of the biggest misconceptions about sex therapy is that it involves sexual activity or physical touch.
It does not.
Sex therapy is simply talk therapy that focuses on concerns related to sexuality, intimacy, relationships, and sexual well-being.
How Can Sex Therapy Help?
Sex therapy can help survivors:
Rebuild a healthy relationship with sexuality.
Reduce shame surrounding sex and their bodies.
Address low sexual desire.
Improve arousal and orgasm difficulties.
Address erectile dysfunction related to trauma.
Heal fear surrounding intimacy.
Improve communication with a partner.
Learn to establish and maintain healthy sexual boundaries.
Reconnect with pleasure in a way that feels safe and authentic.
Treatment always moves at your pace.
There is never pressure to discuss topics before you are ready, and there is never pressure to engage in any type of sexual activity.
The goal is to create a space where healing can happen safely.
Rebuilding Your Relationship With Sexuality
Sexual trauma often changes the meaning of sex.
Instead of feeling connected, pleasurable, or safe, sex may become associated with fear, obligation, shame, anxiety, or danger.
One of the primary goals of sex therapy is helping survivors redefine what sexuality means to them.
Healing often includes exploring questions such as:
What does healthy intimacy look like for me?
What helps me feel emotionally and physically safe?
What are my boundaries?
What do I genuinely enjoy?
How can I communicate my needs confidently?
What kind of sexual relationship do I want moving forward?
These conversations help survivors build a sexuality based on choice rather than survival.
Sex Therapy for Couples
Sexual trauma often affects both the survivor and their intimate relationship.
Partners may struggle to understand trauma responses such as:
Avoiding sex.
Dissociating during intimacy.
Low sexual desire.
Fear of physical touch.
Emotional withdrawal.
Difficulty talking about sex.
Feelings of rejection or confusion.
Sex therapy helps couples understand how trauma affects intimacy while teaching skills that improve communication, trust, emotional safety, and physical connection.
The goal is never to pressure someone into having sex.
The goal is to help both partners create a relationship where intimacy feels safe, consensual, connected, and mutually enjoyable.
Sex Therapy Often Complements Trauma Therapy
For many survivors, the most effective treatment combines trauma therapy with sex therapy.
As treatments such as EMDR help reduce the emotional intensity of traumatic memories, sex therapy helps survivors rebuild confidence, reconnect with their bodies, improve communication, and create healthier experiences of intimacy.
Together, these approaches address both the trauma itself and its impact on sexual health and relationships.
Pelvic Floor Physical Therapy
Sexual trauma can affect more than emotional well-being—it can also affect the muscles of the pelvic floor.
Many survivors experience symptoms such as pain during sex, pelvic pain, difficulty relaxing the pelvic muscles, urinary symptoms, or discomfort during medical exams.
Pelvic floor physical therapists are specially trained to evaluate and treat these concerns using a trauma-informed, patient-centered approach.
Treatment may include:
Education about the pelvic floor muscles.
Gentle relaxation techniques.
Breathing exercises.
Stretching and movement.
Home exercises.
Pain management strategies.
Treatment is always collaborative, and you remain in control throughout the process. A trauma-informed pelvic floor physical therapist will explain each step, ask for your consent, and respect your boundaries.
Pelvic floor physical therapy is often used alongside treatments such as EMDR, sex therapy, and psychotherapy to address both the physical and emotional effects of sexual trauma.
Medication
For some survivors, medication can be a helpful part of recovery from sexual trauma.
While medication cannot erase traumatic memories, it can help reduce symptoms that make healing more difficult, such as anxiety, depression, panic attacks, nightmares, sleep problems, or post-traumatic stress symptoms.
Common medications may include:
Antidepressants (SSRIs or SNRIs).
Anti-anxiety medications.
Medications to help reduce trauma-related nightmares.
Sleep medications, when appropriate.
Medication is often most effective when combined with evidence-based therapies such as EMDR or other trauma-informed treatments.
A psychiatrist or primary care provider can help determine whether medication may be appropriate based on your symptoms and overall health.

Part 9: Rebuilding Intimacy
Reconnecting With Yourself
After sexual trauma, it is common to feel disconnected from yourself, your body, and your sexuality.
Healing begins by rebuilding the relationship you have with yourself before focusing on intimacy with someone else.
This may include learning to trust your instincts, practicing self-compassion, reconnecting with your body, and discovering what makes you feel safe.
The stronger your relationship with yourself becomes, the easier it is to build healthy, connected relationships with others.
Taking Sex Off the Table
Many couples feel pressure to "get back to normal" after sexual trauma.
Sometimes, one of the most healing things you can do is temporarily take sex off the table.
Removing the expectation of sex allows both partners to focus on emotional connection without the pressure of performance or fear.
This creates space to rebuild safety, trust, and closeness before returning to sexual activity.
Sensate Focus
Sensate Focus is an evidence-based exercise developed to help people reconnect with physical touch without pressure or performance.
Partners take turns exploring non-sexual touch while focusing on physical sensations rather than orgasm or intercourse.
The goal is to rebuild comfort, mindfulness, and connection one step at a time.
Many sex therapists use Sensate Focus to help survivors and couples restore safety during intimacy.
Expanding Intimacy Beyond Penetration
Intimacy is much bigger than intercourse.
Many couples discover that emotional closeness, affection, laughter, kissing, cuddling, massage, hand-holding, and meaningful conversations strengthen their relationship just as much as sexual activity.
Expanding your definition of intimacy reduces pressure and reminds both partners that connection can happen in many different ways.
Communicating Boundaries
Healthy boundaries help create emotional and physical safety.
After sexual trauma, it is important to communicate what feels comfortable, what doesn't, and what you need in order to feel safe.
Boundaries are not barriers to intimacy—they are what make healthy intimacy possible.
A caring partner will respect your boundaries without pressure or guilt.
Rebuilding Trust
Trauma can make trusting others feel incredibly difficult.
Trust is rebuilt through consistency, honesty, patience, and respect over time—not through grand gestures.
Healthy partners earn trust by respecting boundaries, listening, following through on their words, and creating emotional safety.
Trust grows one safe experience at a time.
Returning to Sexual Activity
There is no "right" timeline for returning to sexual activity after sexual trauma.
Some survivors feel ready sooner, while others need more time.
The most important question is not, "Should I be having sex yet?"
It is, "Do I feel emotionally and physically safe enough to choose this?"
When you decide to become sexually active again, move slowly, communicate openly, and give yourself permission to pause or stop at any time.
Healing is not measured by how quickly you return to sex.
It is measured by whether intimacy feels like a choice rather than an obligation.

Part 10: What Partners Should Know
How Trauma Affects Relationships
Sexual trauma doesn't just affect the survivor.
It can also affect romantic relationships in ways that neither partner expected.
Many partners want to help but aren't sure what to do. They may feel confused, rejected, helpless, or afraid of saying the wrong thing.
At the same time, survivors often worry that their partner won't understand what they're experiencing.
The good news is that healthy relationships can become an important part of healing.
Understanding how trauma affects intimacy allows couples to respond with compassion instead of confusion.
Trauma Changes the Nervous System
One of the most important things partners can understand is that trauma changes the brain and nervous system.
Many reactions that seem confusing are actually automatic survival responses.
For example, your partner may:
Pull away from physical touch.
Freeze during conflict.
Become emotionally distant.
Feel overwhelmed by intimacy.
Become easily startled.
Need more personal space.
Struggle to relax.
These responses are usually not a reflection of how they feel about you.
They are signs that their nervous system is trying to keep them safe.
It Isn't About You
One of the hardest parts for partners is remembering that trauma responses are rarely personal.
A survivor may decline sex, avoid touch, or become emotionally withdrawn.
It is easy to assume:
"They're not attracted to me."
"I must have done something wrong."
"They don't love me anymore."
In many cases, none of those things are true.
The survivor's brain is responding to past experiences—not to the relationship they have with you today.
Intimacy May Feel Different
After sexual trauma, intimacy may bring up fear, anxiety, shame, or vulnerability.
A survivor may:
Want closeness but fear sexual contact.
Enjoy affection but avoid intercourse.
Need intimacy to move more slowly.
Become triggered unexpectedly.
Have difficulty staying present during sex.
Experience changes in desire or arousal.
These reactions are common after trauma and often improve with time, communication, and appropriate treatment.
Communication Becomes Even More Important
Trauma can make it difficult to talk about needs, boundaries, or fears.
Creating a relationship where both partners can communicate openly is one of the strongest predictors of healing.
Helpful questions include:
"What helps you feel safe?"
"How can I support you?"
"Would you like a hug, or would you prefer space?"
"What feels comfortable for you today?"
Listening without judgment often matters more than having the perfect answer.
Patience Is Part of Healing
Healing rarely follows a straight line.
Some days your partner may feel connected and comfortable.
Other days they may struggle with triggers, anxiety, or emotional distance.
Progress is rarely measured by the absence of difficult days.
It is measured by the growing sense of safety, trust, and connection within the relationship.
Patience allows healing to happen at a pace the nervous system can tolerate.
Your Relationship Can Become Part of the Healing
A healthy relationship cannot erase trauma.
But it can provide something incredibly powerful:
Repeated experiences of safety.
Every respectful conversation.
Every honored boundary.
Every moment of consent.
Every act of kindness.
Every time you respond with patience instead of pressure, you help create a relationship that teaches the nervous system something new:
"I am safe here."
Partners Need Support Too
Supporting someone who has experienced sexual trauma can be emotionally challenging.
Partners may experience sadness, frustration, grief, confusion, or feelings of helplessness.
These emotions are normal.
Taking care of your own mental health, seeking support when needed, and learning about trauma can help you remain a supportive partner without losing yourself in the process.
You do not have to carry the weight of healing alone.
Healing Is a Team Effort
Recovery is not about one partner fixing the other.
It is about two people working together to create a relationship built on safety, respect, communication, and trust.
Many couples discover that while trauma changes their relationship, healing also strengthens it.
They learn to communicate more openly.
Respect boundaries more consistently.
Value emotional intimacy more deeply.
And create a relationship that feels more secure than it did before.
Supporting a Survivor
Loving someone who has experienced sexual trauma can feel overwhelming at times.
You may want to help but worry about saying the wrong thing, making things worse, or not knowing what your partner needs.
The most important thing to remember is this:
You do not have to "fix" your partner.
Your role is to help create a relationship where they feel safe, respected, and supported.
Healing happens through many small experiences of trust, patience, and emotional safety.
Helpful Things to Say
You don't need the perfect words.
Often, simple and genuine statements are the most meaningful.
You might say:
"I'm here for you."
"Thank you for trusting me."
"I believe you."
"You don't have to go through this alone."
"We can go at your pace."
"Your boundaries matter to me."
"What would help you feel safe right now?"
"It's okay if you don't have the words."
"We don't have to do anything you're not comfortable with."
"I care about you whether we have sex or not."
These statements communicate acceptance, patience, and emotional safety.
Things to Avoid
Even well-meaning comments can unintentionally increase shame or pressure.
Try to avoid saying things like:
"You should be over this by now."
"That happened a long time ago."
"I would never hurt you."
"You're overreacting."
"You just need to relax."
"When are we going to have sex again?"
"If you loved me, you would…"
"Everyone has baggage."
"Can't we just move on?"
These statements may minimize the survivor's experience or make them feel responsible for healing on someone else's timeline.
Navigating Consent Together
Consent is more than asking, "Do you want to have sex?"
It is an ongoing conversation built on respect, communication, and choice.
Healthy couples check in with each other regularly.
This might sound like:
"How are you feeling?"
"Does this feel okay?"
"Would you like me to keep going?"
"Would you rather slow down?"
"Do you want to stop?"
Remember that consent can change at any time.
Someone can say yes and later decide they want to pause or stop.
Responding with kindness and respect builds trust.
The goal is not simply getting consent.
The goal is helping your partner feel completely free to say both yes and no.
Patience During Healing
Healing after sexual trauma is rarely quick or predictable.
Some days your partner may feel connected and hopeful.
Other days they may struggle with triggers, anxiety, or emotional distance.
This doesn't mean healing has stopped.
Recovery often happens through many small steps rather than dramatic breakthroughs.
Patience means accepting that healing cannot be rushed.
It means celebrating small victories.
It means understanding that emotional safety is more important than meeting expectations.
The greatest gift you can offer your partner is consistency.
Showing up.
Listening.
Respecting boundaries.
Remaining patient.
Choosing compassion, even on difficult days.
These moments help teach the nervous system something incredibly important:
"This relationship is different."
Healing Together
Healing from sexual trauma does not mean one partner carries all the responsibility.
It is something couples navigate together.
The strongest relationships are built on:
Open communication.
Mutual respect.
Emotional safety.
Healthy boundaries.
Patience.
Curiosity instead of judgment.
Consent.
Compassion.
Many couples discover that as they move through healing together, their relationship becomes stronger, more honest, and more emotionally connected than they ever imagined.

Part 11: Healing Your Relationship With Your Body
Body Image After Trauma
Sexual trauma doesn't just affect how you think about what happened.
It can also change the way you see your body.
Many survivors struggle with body image after trauma, even if they never had concerns before. Some feel disconnected from their bodies. Others feel ashamed, angry, or uncomfortable in their own skin. Some avoid mirrors, dislike being touched, or feel as though their body no longer belongs to them.
If this has been your experience, you are not alone.
Body image struggles are incredibly common after sexual trauma.
The good news is that your relationship with your body can heal.
Why Trauma Affects Body Image
After trauma, many survivors begin viewing their bodies through the lens of what happened to them.
Some people blame their bodies for not fighting harder.
Others feel betrayed by their body's survival responses, physical reactions, or emotional responses during the assault.
Some feel that their body has become a reminder of the trauma.
None of these reactions mean your body failed you.
Your body did exactly what it was designed to do.
It survived.
Common Body Image Struggles After Trauma
Every survivor's experience is different, but common concerns include:
Feeling disconnected from your body.
Feeling ashamed of your body.
Avoiding mirrors.
Feeling uncomfortable being seen naked.
Difficulty accepting compliments.
Feeling unattractive or undesirable.
Feeling like your body isn't yours.
Constantly criticizing your appearance.
Avoiding physical touch.
Feeling anxious during medical exams or intimacy.
These reactions are common trauma responses—not signs that something is wrong with you.
Your Body Is Not the Problem
Trauma often convinces survivors that something is wrong with their body.
In reality, your body is not the source of the problem.
The trauma was.
Your body protected you in the only ways it knew how.
It froze.
It dissociated.
It released stress hormones.
It did everything it could to increase your chances of survival.
Your body deserves gratitude for surviving, not blame for what happened.
Moving From Criticism to Compassion
Healing your body image doesn't require loving your body every single day.
For many survivors, the first step is simply becoming less critical.
Instead of asking:
"How does my body look?"
Try asking:
"What has my body done for me today?"
Perhaps it:
Helped you take a walk.
Hugged someone you love.
Allowed you to laugh.
Helped you breathe.
Carried you through another day.
Your body's value has never been determined by its appearance.
Reconnecting With Your Body
Healing often involves becoming curious about your body again.
You might try:
Gentle stretching.
Yoga.
Walking.
Mindful breathing.
Dancing.
Spending time in nature.
Taking a warm bath.
Applying lotion mindfully.
Wearing clothes that feel comfortable.
Practicing grounding exercises.
The goal isn't to change your body.
The goal is to feel safe living in it.
Challenging Negative Beliefs
Trauma often creates harsh beliefs such as:
"I'm damaged."
"I'm ugly."
"My body betrayed me."
"No one will find me attractive."
"My body isn't safe."
These thoughts often feel true because they've been repeated so many times.
But they are trauma-based beliefs—not objective facts.
Healing involves gradually replacing them with more compassionate truths.
For example:
"My body helped me survive."
"My worth isn't based on my appearance."
"My body deserves kindness."
"I am learning to feel safe again."
Changing these beliefs takes time, but it is possible.
Your Body Belongs to You
One of the deepest wounds of sexual trauma is the loss of control over your own body.
Healing includes reclaiming that ownership.
You get to decide:
Who touches your body.
When you want physical affection.
What feels safe.
What your boundaries are.
How you care for yourself.
Every choice you make reinforces an important truth:
My body belongs to me.
Body Neutrality, Self-Compassion, and Reconnecting With Your Body
Healing after sexual trauma isn't about forcing yourself to love your body.
For many survivors, that goal can feel overwhelming or even impossible.
Instead, healing often begins with something much more achievable:
Learning to treat your body with kindness.
Your body survived something incredibly difficult.
It deserves compassion—not criticism.
What Is Body Neutrality?
Body neutrality is the idea that your worth is not determined by how your body looks.
Instead of focusing on loving every part of your appearance, body neutrality encourages appreciating what your body does for you.
For example, you might begin noticing:
My body helps me breathe.
My body allows me to hug people I love.
My body carries me through each day.
My body has survived incredibly difficult experiences.
My body deserves care and respect.
For many survivors, body neutrality feels more realistic than trying to immediately love a body that has been deeply impacted by trauma.
Practicing Self-Compassion
Trauma often changes the way survivors speak to themselves.
Many people find themselves thinking:
"I'm broken."
"My body failed me."
"I should be over this."
"I'll never feel normal again."
Healing begins by replacing judgment with compassion.
Instead of asking:
"What's wrong with me?"
Try asking:
"What happened to me?"
Or:
"What does my nervous system need right now?"
Speaking to yourself with the same kindness you would offer a close friend helps create the emotional safety needed for healing.
Mindfulness and Movement
Trauma can make it difficult to feel connected to your body.
Mindfulness and gentle movement help rebuild that connection without pressure.
Activities might include:
Walking.
Gentle stretching.
Yoga.
Deep breathing.
Dancing.
Spending time in nature.
Mindful body scans.
The goal isn't exercise or performance.
The goal is simply noticing your body with curiosity instead of judgment.
Each moment of safe movement teaches your nervous system that your body is no longer only associated with danger.
Reconnecting With Pleasure
After sexual trauma, pleasure can feel unfamiliar or even frightening.
It's important to remember that pleasure doesn't have to be sexual.
Healing often begins by rediscovering simple experiences that feel comforting or enjoyable.
This might include:
Feeling sunshine on your skin.
Drinking your favorite coffee or tea.
Wrapping yourself in a soft blanket.
Listening to music.
Taking a warm bath.
Petting a dog or cat.
Smelling fresh flowers.
Laughing with someone you trust.
These everyday moments help remind your brain that your body is capable of experiencing comfort, peace, and joy.
Over time, these experiences create a stronger foundation for reconnecting with sexual pleasure, if and when you choose.
Reclaiming Your Body
Perhaps the greatest part of healing is remembering that your body still belongs to you.
The trauma may have taken away your sense of control for a period of time.
Healing is about taking that control back.
Reclaiming your body may look like:
Choosing who touches you.
Saying yes because you want to.
Saying no without guilt.
Wearing clothes that make you feel comfortable.
Looking at yourself with less criticism.
Caring for your body because it deserves care—not because it needs to change.
Honoring your physical and emotional boundaries.
Every choice you make reinforces an important truth:
"My body belongs to me."
No one can take that truth away.

Part 12: Frequently Asked Questions
Can sexual trauma cause low libido?
Yes.
Many survivors notice changes in sexual desire after trauma. Your brain and nervous system may begin associating sex with fear, danger, or stress rather than pleasure and connection. Low libido is one of the most common effects of sexual trauma, and it does not mean there is something wrong with you. As healing progresses, many people notice that their desire gradually returns.
Can sexual trauma cause painful sex?
Yes.
Sexual trauma can contribute to pain during sex by causing the pelvic floor muscles to tighten, increasing anxiety, reducing arousal, or making it difficult for the body to relax. Painful sex is a common trauma response and can often improve with treatments such as trauma therapy, pelvic floor physical therapy, and sex therapy.
Can sexual trauma cause erectile dysfunction?
Yes.
Sexual trauma can affect people of all genders. Anxiety, hypervigilance, shame, dissociation, and nervous system activation can all interfere with erections. Erectile dysfunction after trauma is not simply "in your head." It is often a very real response of the brain and body trying to stay safe.
Can sexual trauma cause vaginismus?
Yes.
Some survivors develop vaginismus, a condition in which the pelvic floor muscles tighten involuntarily, making penetration painful or impossible. This is an automatic protective response—not something you are choosing. Treatment often includes pelvic floor physical therapy, trauma therapy, and sex therapy.
Can sexual trauma cause difficulty orgasming?
Yes.
Many survivors experience difficulty reaching orgasm after trauma. Anxiety, dissociation, shame, fear, and difficulty feeling present can all interfere with sexual pleasure. Healing often involves rebuilding safety, reconnecting with the body, and reducing the nervous system's need to stay in survival mode.
Why do I dissociate during sex?
Dissociation is a common trauma response.
If your brain associates sexual intimacy with past danger, it may disconnect from the experience to protect you. Dissociation is not a choice or a sign that you don't love your partner. It is your nervous system using a survival strategy that once helped you cope. Trauma-informed treatment can help reduce dissociation over time.
Why do I freeze during sexual assault?
Freezing is one of the body's natural survival responses.
When fighting or escaping doesn't feel possible, the nervous system may automatically shut down movement in an attempt to increase survival. This response happens outside of conscious control. Freezing does not mean you consented, and it is never your fault.
Can EMDR help sexual trauma?
Yes.
EMDR is one of the most researched and effective treatments for trauma. It helps the brain process traumatic memories so they become less emotionally overwhelming. Many survivors notice fewer triggers, reduced anxiety, improved emotional regulation, and greater comfort with intimacy after EMDR therapy.
How long does healing take?
There is no universal timeline.
Healing depends on many factors, including the type of trauma, how long it occurred, available support, and individual differences. Some people notice improvement within months, while others heal over several years. Progress is not measured by speed—it is measured by increased safety, connection, and quality of life.
Can I ever enjoy sex again?
Yes.
Many survivors worry they will never experience pleasure again, but healing is absolutely possible. As your brain and nervous system learn that intimacy can be safe, many people rediscover desire, pleasure, emotional connection, and satisfying sexual relationships. Healing may take time, but a fulfilling sex life is possible.
Is it normal to avoid sex after assault?
Yes.
Avoiding sex after sexual trauma is a very common response. Your brain is trying to protect you from something it believes may be dangerous. Avoiding intimacy does not mean you are broken. As healing progresses and safety increases, many survivors gradually feel more comfortable reconnecting with intimacy.
Can men experience sexual trauma?
Absolutely.
Men, women, transgender, and nonbinary individuals can all experience sexual trauma. Unfortunately, many men struggle in silence because of stigma or myths about masculinity. Sexual trauma can affect anyone, regardless of gender, sexual orientation, or age, and everyone deserves support and healing.
Why do I blame myself?
Self-blame is one of the most common responses after sexual trauma.
Many survivors search for ways they could have prevented what happened because believing they had control can feel less frightening than accepting that someone else chose to harm them. The responsibility always belongs to the person who committed the assault—not the survivor.
Why can't I remember everything?
Trauma affects how memories are stored.
During overwhelming experiences, the brain focuses on survival rather than creating clear, organized memories. As a result, many survivors have memory gaps or fragmented memories. This is a normal effect of trauma and does not mean you are making it up or that your experience was not real.
Is hypersexuality a trauma response?
It can be.
While some survivors avoid sex after trauma, others experience increased sexual thoughts or behaviors. For some people, sex becomes a way to cope with difficult emotions, regain a sense of control, seek connection, or numb emotional pain. Neither response is "right" or "wrong." Both can be understandable adaptations to trauma.
Does everyone develop PTSD after sexual trauma?
No.
While many survivors develop symptoms of post-traumatic stress, not everyone meets the criteria for PTSD. Some people experience anxiety, depression, changes in sexuality, relationship difficulties, or other trauma-related symptoms without developing PTSD. Every survivor responds differently, and every response is valid.
Can therapy still help years later?
Yes.
It is never too late to heal.
Many people begin trauma therapy years—or even decades—after their experiences and still make meaningful progress. Because the brain remains capable of change throughout life, evidence-based treatments such as EMDR, sex therapy, and other trauma-informed approaches can be effective no matter how much time has passed since the trauma.
Part 13: Key Takeaways
You've just read a great deal of information about sexual trauma, how it affects the brain and body, and what healing can look like.
If you remember only a few things from this guide, let them be these.
1. What Happened to You Was Not Your Fault
No matter what you wore.
No matter how much you drank.
No matter whether you froze.
No matter whether you fought back.
No matter whether you knew the person.
No matter what happened afterward.
The responsibility always belongs to the person who chose to violate your consent.
2. Your Reactions Make Sense
Difficulty orgasming.
Dissociation.
Hypervigilance.
Avoiding intimacy.
Hypersexuality.
Triggers.
Emotional numbness.
These are not signs that you are broken.
They are common survival responses to trauma.
Your brain and nervous system adapted to help you survive.
3. Your Brain and Body Can Heal
One of the most hopeful discoveries in neuroscience is that the brain can change throughout life.
Through neuroplasticity, your nervous system can learn that the danger is over.
Healing happens through repeated experiences of safety, support, and connection.
Recovery is possible.
4. Healing Takes Time
There is no correct timeline.
Some people heal quickly.
Others heal over years.
Neither path is better than the other.
Healing is not a race.
Every step forward matters.
5. Healing Is Not Linear
There will be good days.
There will be difficult days.
You may feel strong one week and overwhelmed the next.
Setbacks do not erase your progress.
Healing is measured over time, not by a single moment.
6. You Deserve Safe Relationships
Healthy relationships are built on:
Respect.
Consent.
Communication.
Trust.
Patience.
Emotional safety.
You deserve relationships where your boundaries are honored and your voice matters.
7. Your Body Is Not the Enemy
Your body did not betray you.
It protected you.
Every survival response—whether you fought, fled, froze, fawned, or dissociated—was your nervous system doing everything it could to keep you alive.
Your body deserves compassion.
8. Healing Is About More Than Reducing Symptoms
Recovery is not simply having fewer triggers.
Healing also means:
Feeling safe in your body.
Trusting yourself again.
Building healthy relationships.
Setting boundaries.
Experiencing joy.
Feeling present.
Reconnecting with intimacy.
Living a life that is no longer controlled by trauma.
9. You Do Not Have to Heal Alone
Healing is often easier with support.
Trauma-informed therapists, EMDR therapists, sex therapists, pelvic floor physical therapists, supportive medical providers, trusted friends, and healthy relationships can all play important roles in recovery.
Asking for help is a sign of strength, not weakness.
10. Healing Is Possible
Perhaps the most important message in this entire guide is this:
Healing is possible.
Not because what happened didn't matter.
Not because you'll forget.
Not because the pain disappears overnight.
But because your brain can heal.
Your body can learn safety again.
Your relationships can become healthy.
Your sexuality can become yours again.
Your future does not have to be defined by your past.
Part 14: Next Steps If You're Ready for Help
When to Seek Professional Support
Healing from sexual trauma is not something you have to do alone.
While some survivors find that symptoms gradually improve with time, others continue to struggle with anxiety, triggers, relationship difficulties, or changes in their sexuality long after the trauma occurred.
If your symptoms are interfering with your daily life, your relationships, or your ability to feel safe, it may be time to reach out for professional support.
Seeking therapy is not a sign that you are weak.
It is a sign that you are ready to invest in your healing.
Signs You May Benefit From Therapy
You don't need to be in crisis to benefit from therapy.
You may find therapy helpful if you:
Feel anxious or on edge much of the time.
Experience flashbacks or nightmares.
Avoid people, places, or situations that remind you of the trauma.
Feel disconnected from your body or emotions.
Dissociate during intimacy or everyday life.
Struggle with trust or relationships.
Experience low sexual desire, pain during sex, erectile dysfunction, or difficulty reaching orgasm.
Feel overwhelmed by shame, guilt, or self-blame.
Notice that your trauma is affecting your work, school, parenting, or friendships.
Feel stuck, even though the trauma happened months or years ago.
You do not have to wait until things get worse before asking for help.
What to Look for in a Therapist
Not every therapist specializes in trauma or sexual health.
If possible, look for someone with training in trauma-informed care and evidence-based treatments.
You may want to ask whether they have experience with:
Sexual trauma.
PTSD and complex trauma.
EMDR.
Dissociation.
LGBTQ+ affirming care, if that is important to you.
Pelvic pain or sexual health concerns, when appropriate.
The relationship you have with your therapist matters.
You should feel respected, heard, and emotionally safe.
It's Okay to Ask Questions
Your first therapy appointment is an opportunity to decide whether the therapist feels like a good fit.
Some questions you might ask include:
What experience do you have working with sexual trauma?
What approaches do you use in treatment?
How do you help clients feel safe during therapy?
What can I expect during the first few sessions?
How do you know when someone is ready to process trauma?
A good therapist will welcome these questions and be happy to explain their approach.
You Don't Have to Tell Your Whole Story Right Away
Many survivors worry that starting therapy means immediately talking about the trauma in detail.
That is not how trauma-informed therapy works.
Most therapists begin by helping you build coping skills, emotional regulation, and a sense of safety before processing difficult memories.
You are in control of your healing.
You decide what you share and when you are ready to share it.
Finding the Right Therapist
Taking the first step toward therapy can feel overwhelming.
You may wonder how to find someone who understands sexual trauma or worry about whether therapy will actually help.
Finding the right therapist is one of the most important parts of the healing process.
The right therapist should help you feel safe, respected, heard, and never pressured.
Remember, you are interviewing the therapist just as much as they are getting to know you.
You deserve someone who is a good fit.
Finding a Trauma-Informed Therapist
Not every therapist has specialized training in trauma.
A trauma-informed therapist understands how trauma affects the brain, nervous system, body, relationships, and emotions.
Rather than asking, "What's wrong with you?" they ask, "What happened to you?"
When looking for a therapist, consider asking:
Do you specialize in trauma?
What training have you received in treating trauma?
How do you help clients feel emotionally safe?
What trauma therapies do you use?
Do you have experience working with survivors of sexual trauma?
A trauma-informed therapist will respect your boundaries, move at your pace, and never pressure you to discuss traumatic experiences before you feel ready.
Finding an EMDR Therapist
If you are interested in EMDR, look for a therapist who has completed formal EMDR training through an approved EMDR training program.
Many therapists list EMDR on their websites, but it's okay to ask about their experience.
Questions you might ask include:
How long have you been practicing EMDR?
How often do you use EMDR in your practice?
Have you worked with survivors of sexual trauma?
How do you prepare clients before beginning trauma processing?
A qualified EMDR therapist will spend time helping you build coping skills and emotional safety before beginning to process traumatic memories.
Finding a Sex Therapist
If sexual trauma has affected your intimacy, desire, relationships, or sexual functioning, working with a sex therapist may also be helpful.
Sex therapists receive specialized training in human sexuality and understand how trauma can affect sexual well-being.
A sex therapist can help with concerns such as:
Low libido.
Pain during sex.
Erectile dysfunction.
Difficulty reaching orgasm.
Fear of intimacy.
Communication with a partner.
Rebuilding a healthy relationship with sexuality.
It's important to know that sex therapy is talk therapy.
There is never any sexual activity, physical touch, or nudity involved during sessions.
If you're looking for a therapist with specialized training, you may want to find someone who is certified by or working toward certification through the American Association of Sexuality Educators, Counselors and Therapists (AASECT).
What to Expect During Your First Session
Many people worry that the first therapy session will involve sharing every detail of their trauma.
In most cases, it doesn't.
Your first session is usually focused on getting to know you and understanding what brings you to therapy.
Your therapist may ask questions about:
Your current concerns.
Your symptoms.
Your relationships.
Your goals for therapy.
Your support system.
Your medical and mental health history.
You are always in control of what you choose to share.
If something feels too difficult to discuss, it's okay to say so.
A trauma-informed therapist will respect your boundaries.
The first few sessions are often spent building trust, learning coping skills, and creating a sense of safety before processing traumatic memories.
Therapy is not about forcing you to relive your trauma.
It is about helping you heal from it.
Finding the Right Fit
Not every therapist will be the right fit, and that's okay.
If you don't feel safe, understood, or comfortable with a therapist, you have every right to look for someone else.
The therapeutic relationship is one of the strongest predictors of successful treatment.
You deserve someone who:
Listens without judgment.
Respects your boundaries.
Makes you feel emotionally safe.
Has experience treating sexual trauma.
Moves at your pace.
Believes in your ability to heal.
Finding the right therapist may take time, but it is worth the effort.
Healing Starts With One Conversation
Beginning therapy can feel intimidating.
Many survivors worry they'll be judged, won't know what to say, or will become overwhelmed.
Those fears are completely understandable.
Remember, you don't have to tell your entire story during your first appointment.
You don't have to have everything figured out.
You simply have to show up.
Healing doesn't begin because you have all the answers.
It begins because you were willing to take the first step.
About the Author
Holly Nelson is a Licensed Professional Counselor, trauma therapist, and sex therapist (AASECT certification in progress) based in Scottsdale, Arizona. She specializes in helping adults heal from sexual trauma, improve intimacy, navigate relationship challenges, and overcome concerns related to sexual health.
Holly has extensive training in Eye Movement Desensitization and Reprocessing (EMDR), an evidence-based treatment for trauma, and integrates trauma-informed, compassionate care into every aspect of her work. She believes healing is possible when people feel safe, understood, and empowered to move at their own pace.
Her clinical specialties include:
Childhood sexual abuse.
Relationship and intimacy concerns.
Dissociation and nervous system regulation.
Through her private practice, Holly helps individuals and couples reconnect with themselves, their bodies, and their relationships after trauma. Her approach combines neuroscience, evidence-based therapy, and genuine compassion to help clients move beyond survival and create lives filled with safety, connection, and joy.
In addition to providing therapy, Holly is passionate about making accurate, trauma-informed sexual health education accessible to everyone. Through her social media platforms, podcast, workshops, and educational resources, she works to reduce shame, challenge misinformation, and help people understand that healthy sexuality is something everyone deserves
If this guide has helped you better understand yourself or someone you love, Holly hopes it serves as a reminder that healing is possible—and that you do not have to walk that journey alone.
Book your first appointment!
Connect with Holly
Website: www.theconnectioncouch.com
Instagram: @sextherapywithholly
TikTok: @sextherapywithholly
YouTube: @sextherapywithholly
Additional Resources
Healing from sexual trauma can feel overwhelming, but there are many organizations, books, and directories dedicated to helping survivors find support.
If you're ready to take the next step, these resources are excellent places to begin.
Crisis Support
RAINN (Rape, Abuse & Incest National Network)
RAINN is the largest anti-sexual violence organization in the United States. They provide confidential support, educational resources, and a 24/7 crisis hotline.
Website: https://www.rainn.org
National Sexual Assault Hotline:
800-656-HOPE (4673)
Online chat is also available through their website.
988 Suicide & Crisis Lifeline
If you are experiencing thoughts of suicide, overwhelming emotional distress, or are in crisis, help is available 24 hours a day.
Website:
https://988lifeline.org
SAMHSA National Helpline
A free, confidential treatment referral and information service for individuals and families facing mental health or substance use concerns.
Website:
https://www.samhsa.gov
References
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.; DSM-5-TR). American Psychiatric Publishing.
American Psychological Association. (2017). Clinical practice guideline for the treatment of posttraumatic stress disorder (PTSD) in adults.
Briere, J., & Scott, C. (2024). Principles of trauma therapy: A guide to symptoms, evaluation, and treatment (3rd ed.). SAGE Publications.
Courtois, C. A., & Ford, J. D. (Eds.). (2016). Treatment of complex trauma: A sequenced, relationship-based approach. Guilford Press.
Foa, E. B., Hembree, E. A., & Rothbaum, B. O. (2019). Prolonged exposure therapy for PTSD: Emotional processing of traumatic experiences (2nd ed.). Oxford University Press.
International Society for Traumatic Stress Studies. (2019). Posttraumatic stress disorder prevention and treatment guidelines.
Levine, P. A. (2010). In an unspoken voice: How the body releases trauma and restores goodness. North Atlantic Books.
Ogden, P., Minton, K., & Pain, C. (2006). Trauma and the body: A sensorimotor approach to psychotherapy. W. W. Norton & Company.
Porges, S. W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation. W. W. Norton & Company.
Rothschild, B. (2000). The body remembers: The psychophysiology of trauma and trauma treatment. W. W. Norton & Company.
Shapiro, F. (2018). Eye Movement Desensitization and Reprocessing (EMDR) therapy: Basic principles, protocols, and procedures (3rd ed.). Guilford Press.
Siegel, D. J. (2020). The developing mind: How relationships and the brain interact to shape who we are (3rd ed.). Guilford Press.
van der Hart, O., Nijenhuis, E. R. S., & Steele, K. (2006). The haunted self: Structural dissociation and the treatment of chronic traumatization. W. W. Norton & Company.
van der Kolk, B. A. (2015). The body keeps the score: Brain, mind, and body in the healing of trauma. Penguin Books.
World Health Organization. (2013). Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines.
World Health Organization. (2023). Guidelines for the management of conditions specifically related to stress.
References for Sexual Health
American Association of Sexuality Educators, Counselors and Therapists (AASECT). Practice standards and professional resources.
Basson, R. (2001). Using a different model for female sexual response to address women's problematic low sexual desire. Journal of Sex & Marital Therapy, 27(5), 395–403.
International Society for the Study of Women's Sexual Health (ISSWSH). Clinical practice guidelines.
Leiblum, S. R. (Ed.). (2007). Principles and practice of sex therapy (4th ed.). Guilford Press.
Perelman, M. A. (2009). Sex coaching for physicians: Combination treatment for patient and partner. International Journal of Impotence Research, 21, 145–157.
References for Pelvic Floor Physical Therapy
American Physical Therapy Association Academy of Pelvic Health Physical Therapy. Clinical resources and practice guidelines.
Reissing, E. D., Binik, Y. M., Khalifé, S., Cohen, D., & Amsel, R. (2004). Vaginismus, dyspareunia, and pelvic floor muscle function. Journal of Sex & Marital Therapy, 30(1), 5–17.